Department of Internal Medicine III, Cardiology, Angiology and Intensive Care Medicine, University Hospital Schleswig-Holstein Kiel, Kiel, Germany.
Partner Site Hamburg/Kiel/Lübeck, German Centre for Cardiovascular Research, Kiel, Germany.
J Cachexia Sarcopenia Muscle. 2021 Jun;12(3):577-585. doi: 10.1002/jcsm.12689. Epub 2021 Mar 25.
Malnutrition is a hallmark of frailty, is common among elderly patients, and is a predictor of poor outcomes in patients with severe symptomatic aortic stenosis (AS). The Geriatric Nutritional Risk Index (GNRI) is a simple and well-established screening tool to predict the risk of morbidity and mortality in elderly patients. In this study, we evaluated whether GNRI may be used in the risk stratification and management of patients undergoing transcatheter aortic valve replacement (TAVR).
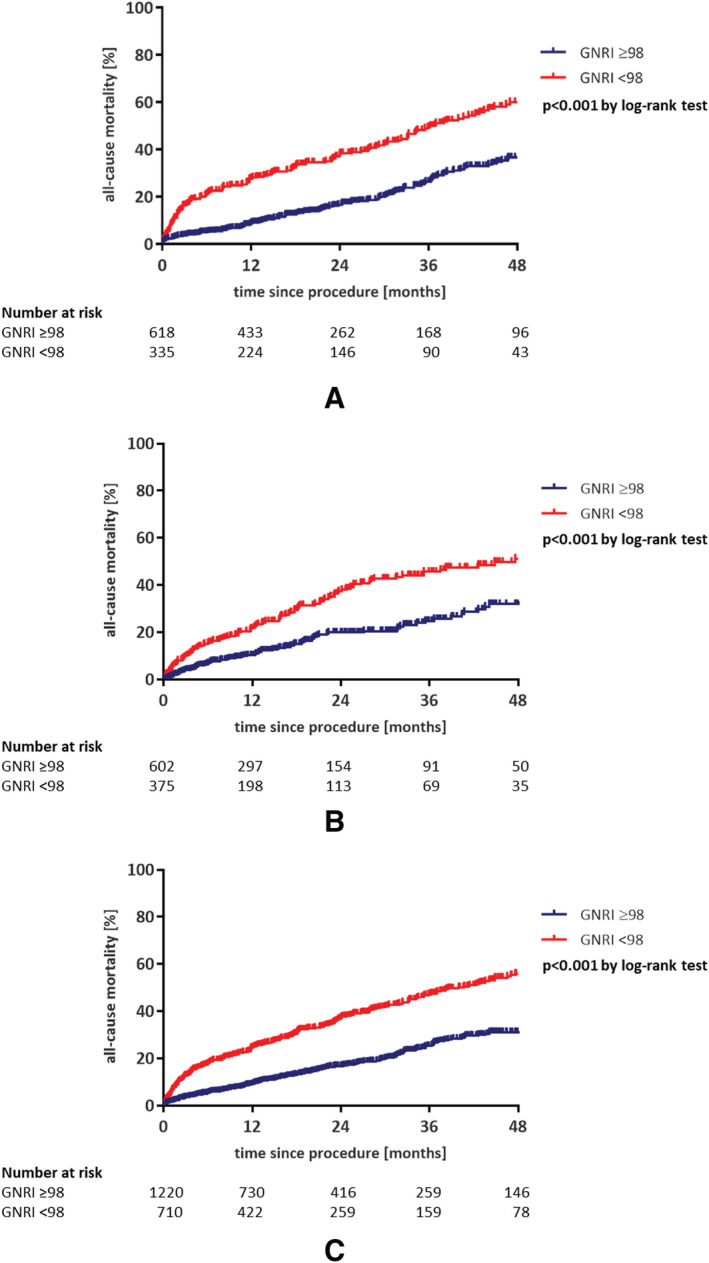
Patients with symptomatic severe AS (n = 953) who underwent transfemoral TAVR at the University Hospital Schleswig-Holstein Kiel, Germany, between 2010 and 2019 (development cohort) were divided into two groups: normal GNRI ≥ 98 (no nutrition-related risk; n = 618) versus low GNRI < 98 (at nutrition-related risk; n = 335). The results were validated in an independent (validation) cohort from another high-volume TAVR centre (n = 977).
The low-GNRI group had a higher proportion of female patients (59.1% vs. 52.1%), higher median age (82.9 vs. 81.8 years), prevalence of atrial fibrillation (50.4% vs. 40.0%), median logistic EuroSCORE (17.5% vs. 15.0%) and impaired left ventricular function (<35%: 10.7% vs. 6.8%), lower median estimated glomerular filtration rate (50 vs. 57 mL/min/1.73 m ) and median albumin level (3.5 vs. 4.0 g/dL) compared with the normal-GNRI group. Among peri-procedural complications, Acute Kidney Injury Network (AKIN) Stage 3 was more common in the low-GNRI group (3.6% vs. 0.6%, p = 0.002). After a mean follow-up of 21.1 months, all-cause mortality was significantly increased in the low-GNRI group compared with the normal-GNRI group (p < 0.001). This was confirmed in the validation cohort (p < 0.001). Low GNRI < 98 was identified as an independent risk factor for all-cause mortality (hazard ratio 1.44, 95% CI 1.01-2.04, p = 0.043). Other independent risk factors included albumin level < median of 4.0 g/dL, high-sensitive troponin T in the highest quartile (> 45.0 pg/mL), N-terminal pro-B-type natriuretic peptide in the highest quartile (> 3595 pg/mL), grade III-IV tricuspid regurgitation, pulmonary arterial hypertension, life-threatening bleeding, AKIN Stage 3 and disabling stroke.
Low GNRI score was associated with an increased risk of all-cause mortality in patients undergoing TAVR, implying that this vulnerable group may benefit from improved preventive measures.
营养不良是衰弱的标志,在老年患者中很常见,也是严重有症状主动脉瓣狭窄(AS)患者不良结局的预测指标。老年营养风险指数(GNRI)是一种简单且经过充分验证的筛查工具,可预测老年患者的发病率和死亡率风险。在本研究中,我们评估了 GNRI 是否可用于行经股动脉主动脉瓣置换术(TAVR)患者的风险分层和管理。
2010 年至 2019 年,德国石勒苏益格-荷尔斯泰因基尔大学医院对 953 例有症状的严重 AS 患者进行了经股 TAVR(发展队列),并将其分为两组:GNRI 正常(≥98;无营养相关风险;n=618)与 GNRI 低(<98;存在营养相关风险;n=335)。研究结果在另一家高容量 TAVR 中心的独立(验证)队列中得到验证(n=977)。
低 GNRI 组女性患者比例较高(59.1% vs. 52.1%),中位年龄较大(82.9 岁 vs. 81.8 岁),心房颤动患病率较高(50.4% vs. 40.0%),中位 logistic EuroSCORE(17.5% vs. 15.0%)和左心室功能受损(<35%:10.7% vs. 6.8%),估计肾小球滤过率中位数较低(50 比 57 mL/min/1.73 m )和白蛋白水平中位数较低(3.5 比 4.0 g/dL)。在围手术期并发症中,低 GNRI 组急性肾损伤网络(AKIN)3 期更为常见(3.6% vs. 0.6%,p=0.002)。平均随访 21.1 个月后,低 GNRI 组的全因死亡率明显高于 GNRI 正常组(p<0.001)。这在验证队列中得到了证实(p<0.001)。低 GNRI<98 是全因死亡率的独立危险因素(危险比 1.44,95%CI 1.01-2.04,p=0.043)。其他独立危险因素包括白蛋白水平<中位数 4.0 g/dL、最高四分位数的高敏肌钙蛋白 T(>45.0 pg/mL)、最高四分位数的 N 末端 pro-B 型利钠肽(>3595 pg/mL)、III 级或 IV 级三尖瓣反流、肺动脉高压、危及生命的出血、AKIN 3 期和致残性中风。
低 GNRI 评分与 TAVR 患者全因死亡率增加相关,这意味着该脆弱人群可能受益于改善的预防措施。