Department of Epidemiology and Biostatistics, Institute of Public Health, College of Medicine and Health Science, University of Gondar, Gondar, Ethiopia.
Department of Human Physiology, School of Medicine, College of Medicine and Health Science, University of Gondar, Gondar, Ethiopia.
PLoS One. 2021 Mar 25;16(3):e0248637. doi: 10.1371/journal.pone.0248637. eCollection 2021.
Childhood undernutrition is the leading cause of under-five mortality and morbidity in the world particularly in East African countries. Although there are studies on child undernutrition in different East African countries, our search of the literature revealed that there is limited evidence of a pooled analysis of these studies. Therefore, this study aimed to investigate the pooled prevalence and associated factors of chronic undernutrition (i.e. stunting) among under-five children in East Africa.
A pooled analysis of the Demographic and Health Surveys (DHSs) in 12 East African countries was conducted. A total weighted sample of 79744 under-five children was included in the study. Mixed-effect logistic regression analysis was used to identify significant factors associated with chronic undernutrition since the DHS data has a hierarchical structure. The intra-class correlation coefficient (ICC), Median Odds Ratio (MOR), Likelihood Ratio (LR)-test, and deviance was used for model comparison. Variables with p-value <0.2 in the bivariable mixed-effect logistic regression analysis were considered for the multivariable analysis. In the multivariable multilevel analysis model, the Adjusted Odds Ratio (AOR) with the 95% Confidence Interval (CI) were reported for significant factors.
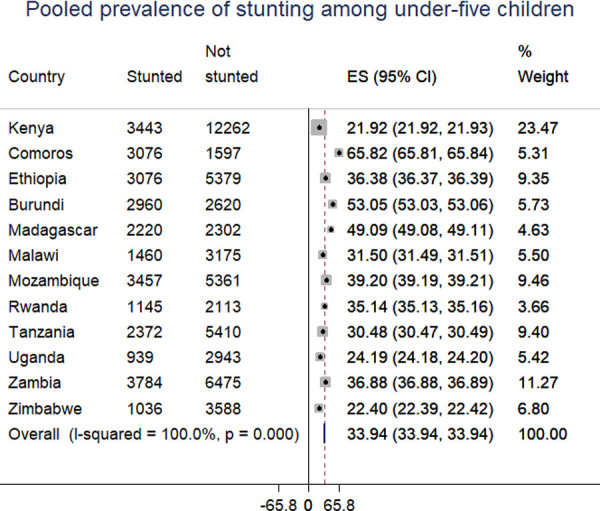
The pooled prevalence of chronic undernutrition among underfive children in East Africa was 33.3% (95% CI: 32.9%, 35.6%) ranging from 21.9% in Kenya to 53% in Burundi. Children whose mothers lived in rural area (AOR = 1.11, 95% CI: 1.06, 1.16), born to mother who had no formal education (AOR = 1.42, 95% CI: 1.34, 1.50) and primary education (AOR = 1.37, 95% CI: 1.31, 1.44), being in poor household (AOR = 1.66, 95% CI: 1.58, 1.74), and middle household (AOR = 1.42, 95% CI: 1.35, 1.49), child aged 36-48 months (AOR = 1.09, 95% CI: 1.04, 1.14), being male (AOR = 1.19, 95% CI: 1.15, 1.23), 2nd - 4th birth order (AOR = 1.08, 95% CI: 1.03, 1.13), and above 4th 1.27 (AOR = 1.27, 95% CI: 1.19, 1.35), home delivery 1.09 (AOR = 1.09, 95% CI: 1.05, 1.13), small size at birth (AOR = 1.35, 95% CI: 1.29, 1.40) and being multiple births (AOR = 1.98, 95% CI: 1.81, 2.17) were associated with increased odds of stunting. While, antenatal care visit (AOR = 0.89, 95% CI: 0.86, 0.93), mothers aged 25-34 (AOR = 0.83, 95% CI: 0.79, 0.86) and ≥ 35 years (AOR = 0.76, 95% CI: 0.72, 0.81), large size at birth (AOR = 0.85, 95% CI: 0.81, 0.88), and family size >8 (AOR = 0.92, 95% CI: 0.87, 0.98) were associated with decreased odds of stunting.
The study revealed that stunting among under-five children remains a major public health problem in East Africa. Therefore, to improve child nutrition status the governmental and non-governmental organizations should design public health interventions targeting rural residents, and the poorest households. Furthermore, enhancing health facility delivery, ANC visit, and maternal health education is vital for reducing child chronic undernutrition.
儿童期营养不良是全世界五岁以下儿童死亡和发病的主要原因,尤其是在东非国家。尽管针对不同的东非国家进行了儿童营养不良方面的研究,但我们对文献的搜索结果表明,对这些研究进行汇总分析的证据有限。因此,本研究旨在调查东非地区五岁以下儿童慢性营养不良(即发育迟缓)的综合患病率及其相关因素。
对 12 个东非国家的人口与健康调查(DHS)进行了汇总分析。研究共纳入了 79744 名五岁以下儿童的加权总样本。由于 DHS 数据具有分层结构,因此采用混合效应逻辑回归分析来确定与慢性营养不良相关的显著因素。使用组内相关系数(ICC)、中位数优势比(MOR)、似然比(LR)检验和偏差来比较模型。在双变量混合效应逻辑回归分析中,p 值<0.2 的变量被认为是多变量分析的候选因素。在多变量多水平分析模型中,报告了有统计学意义的因素的调整优势比(AOR)及其 95%置信区间(CI)。
东非地区五岁以下儿童慢性营养不良的综合患病率为 33.3%(95%CI:32.9%,35.6%),范围从肯尼亚的 21.9%到布隆迪的 53%。母亲居住在农村地区(AOR=1.11,95%CI:1.06,1.16)、母亲未接受过正规教育(AOR=1.42,95%CI:1.34,1.50)和小学教育(AOR=1.37,95%CI:1.31,1.44)、家庭贫困(AOR=1.66,95%CI:1.58,1.74)、中等家庭(AOR=1.42,95%CI:1.35,1.49)、年龄在 36-48 个月(AOR=1.09,95%CI:1.04,1.14)、男性(AOR=1.19,95%CI:1.15,1.23)、第二个到第四个出生顺序(AOR=1.08,95%CI:1.03,1.13)和第四个以上出生(AOR=1.27,95%CI:1.19,1.35)、在家分娩(AOR=1.09,95%CI:1.05,1.13)、出生时体型较小(AOR=1.35,95%CI:1.29,1.40)和多胎(AOR=1.98,95%CI:1.81,2.17)的儿童,其发育迟缓的可能性更高。而接受产前保健(AOR=0.89,95%CI:0.86,0.93)、母亲年龄在 25-34 岁(AOR=0.83,95%CI:0.79,0.86)和≥35 岁(AOR=0.76,95%CI:0.72,0.81)、出生时体型较大(AOR=0.85,95%CI:0.81,0.88)和家庭规模较大(AOR=0.92,95%CI:0.87,0.98)的儿童,其发育迟缓的可能性较低。
本研究表明,东非地区五岁以下儿童的发育迟缓仍然是一个主要的公共卫生问题。因此,为了改善儿童营养状况,政府和非政府组织应该设计针对农村居民和最贫困家庭的公共卫生干预措施。此外,加强卫生机构的分娩服务、产前保健访问和母婴健康教育对于减少儿童慢性营养不良至关重要。