Chen Bo, Gu Hong-Qiu, Liu 刘艺 Yi, Zhang Guqin, Yang Hang, Hu Huifang, Lu Chenyang, Li Yang, Wang Liyi, Liu 刘毅 Yi, Zhao Yi, Pan Huaqin
Department of Rheumatology and Immunology, West China Hospital, Sichuan University, Chengdu, Sichuan, China.
National Center for Healthcare Quality Management in Neurological Diseases, Beijing Tiantan Hospital, Capital Medical University, Beijing, China.
Comput Struct Biotechnol J. 2021;19:1694-1700. doi: 10.1016/j.csbj.2021.03.012. Epub 2021 Mar 22.
To investigate and select the useful prognostic parameters to develop and validate a model to predict the mortality risk for severely and critically ill patients with the coronavirus disease 2019 (COVID-19).
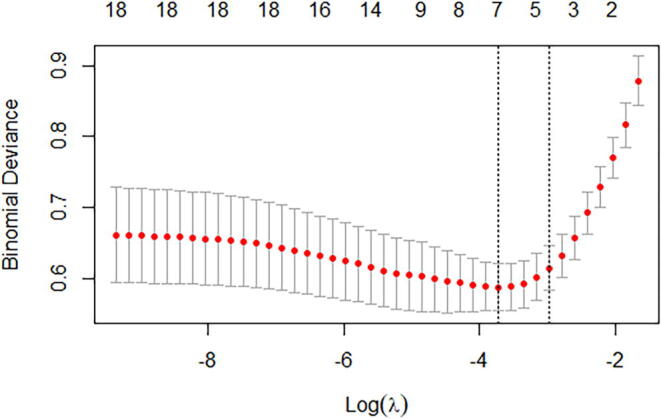
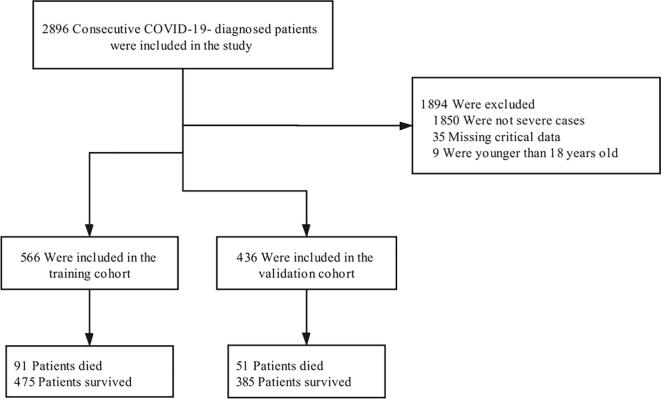
We established a retrospective cohort of patients with laboratory-confirmed COVID-19 (≥18 years old) from two tertiary hospitals: the People's Hospital of Wuhan University and Leishenshan Hospital between February 16, 2020, and April 14, 2020. The diagnosis of the cases was confirmed according to the WHO interim guidance. The data of consecutive severely and critically ill patients with COVID-19 admitted to these hospitals were analyzed. A total of 566 patients from the People's Hospital of Wuhan University were included in the training cohort and 436 patients from Leishenshan Hospital were included in the validation cohort. The least absolute shrinkage and selection operator (LASSO) and multivariable logistic regression were used to select the variables and build the mortality risk prediction model.
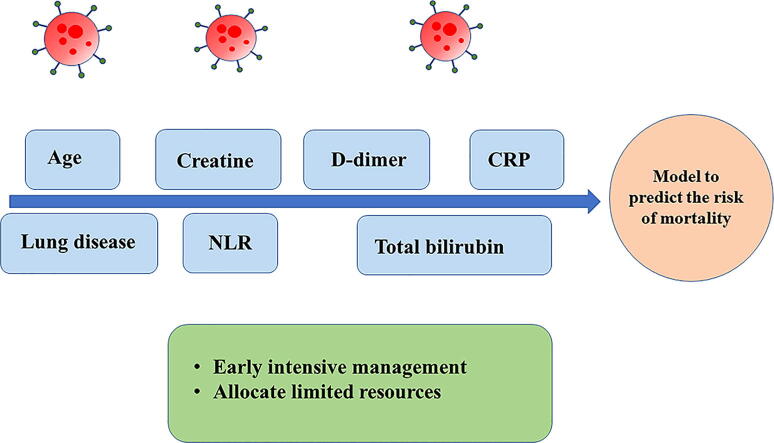
The prediction model was presented as a nomograph and developed based on identified predictors, including age, chronic lung disease, C-reactive protein (CRP), D-dimer levels, neutrophil-to-lymphocyte ratio (NLR), creatinine, and total bilirubin. In the training cohort, the model displayed good discrimination with an AUC of 0.912 [95% confidence interval (CI): 0.884-0.940] and good calibration (intercept = 0; slope = 1). In the validation cohort, the model had an AUC of 0.922 [95% confidence interval (CI): 0.891-0.953] and a good calibration (intercept = 0.056; slope = 1.161). The decision curve analysis (DCA) demonstrated that the nomogram was clinically useful.
A risk score for severely and critically ill COVID-19 patients' mortality was developed and externally validated. This model can help clinicians to identify individual patients at a high mortality risk.
研究并筛选有用的预后参数,以建立并验证一个预测2019冠状病毒病(COVID-19)重症和危重症患者死亡风险的模型。
我们建立了一个回顾性队列,纳入了2020年2月16日至2020年4月14日期间来自两家三级医院(武汉大学人民医院和雷神山医院)实验室确诊的COVID-19患者(≥18岁)。病例诊断依据世界卫生组织临时指南确定。对这些医院收治的连续性COVID-19重症和危重症患者的数据进行分析。武汉大学人民医院的566例患者纳入训练队列,雷神山医院的436例患者纳入验证队列。采用最小绝对收缩和选择算子(LASSO)及多变量逻辑回归来选择变量并建立死亡风险预测模型。
预测模型以列线图形式呈现,并基于确定的预测因子建立,这些预测因子包括年龄、慢性肺病、C反应蛋白(CRP)、D-二聚体水平、中性粒细胞与淋巴细胞比值(NLR)、肌酐和总胆红素。在训练队列中,该模型显示出良好的区分度,曲线下面积(AUC)为0.912 [95%置信区间(CI):0.884 - 0.940],且校准良好(截距 = 0;斜率 = 1)。在验证队列中,该模型的AUC为0.922 [95%置信区间(CI):0.891 - 0.953],校准良好(截距 = 0.056;斜率 = 1.161)。决策曲线分析(DCA)表明该列线图具有临床实用性。
建立了COVID-19重症和危重症患者死亡风险评分并进行了外部验证。该模型可帮助临床医生识别死亡风险高的个体患者。