Grodecki Kajetan, Lin Andrew, Cadet Sebastien, McElhinney Priscilla A, Razipour Aryabod, Chan Cato, Pressman Barry, Julien Peter, Maurovich-Horvat Pal, Gaibazzi Nicola, Thakur Udit, Mancini Elisabetta, Agalbato Cecilia, Menè Roberto, Parati Gianfranco, Cernigliaro Franco, Nerlekar Nitesh, Torlasco Camilla, Pontone Gianluca, Slomka Piotr J, Dey Damini
Biomedical Imaging Research Institute, Cedars-Sinai Medical Center, Los Angeles, CA, USA (K.G., A.L., P.A.M., A.R., D.D.); Monash Health, Melbourne, Australia (A.L., U.T., N.N.); Department of Imaging, Cedars-Sinai Medical Center (S.C., C.C., B.P., P.J.); Department of Radiology, Semmelweis University, Budapest, Hungary (P.M.); Cardiology, Azienda Ospedaliero-Universitaria di Parma, Parma Italy (N.G.); Centro Cardiologico Monzino IRCCS, University of Milan, Italy (E.M., C.A., G.P.); Department of Cardiovascular, Neural and Metabolic Sciences, IRCCS Istituto Auxologico Italiano, Milan, Italy; Department of Medicine and Surgery, University of Milano-Bicocca, Italy (R.M., G.P., F.C., C.T.); Artificial Intelligence in Medicine Program, Cedars-Sinai Medical Center, Los Angeles, CA, USA (P.J.S.).
Radiol Cardiothorac Imaging. 2020 Oct 1;2(5):e200389. doi: 10.1148/ryct.2020200389. eCollection 2020 Oct.
To examine the independent and incremental value of CT-derived quantitative burden and attenuation of COVID-19 pneumonia for the prediction of clinical deterioration or death.
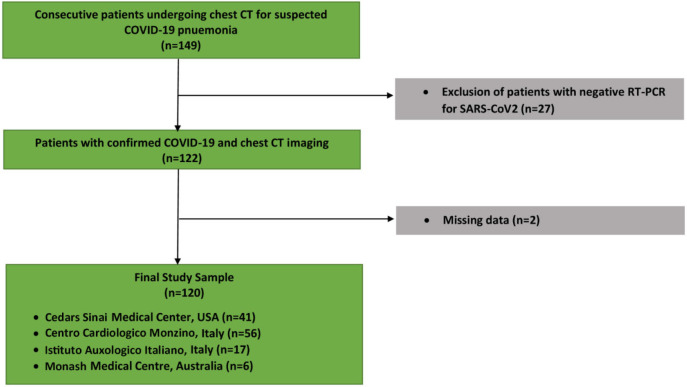
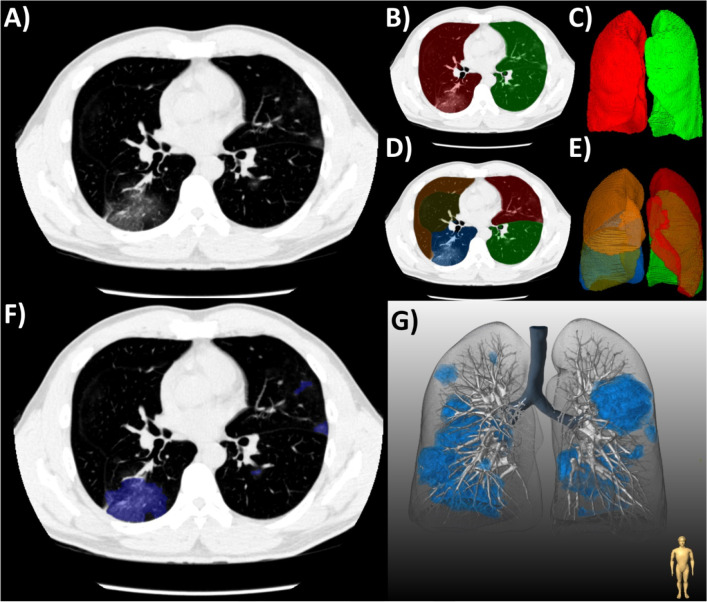
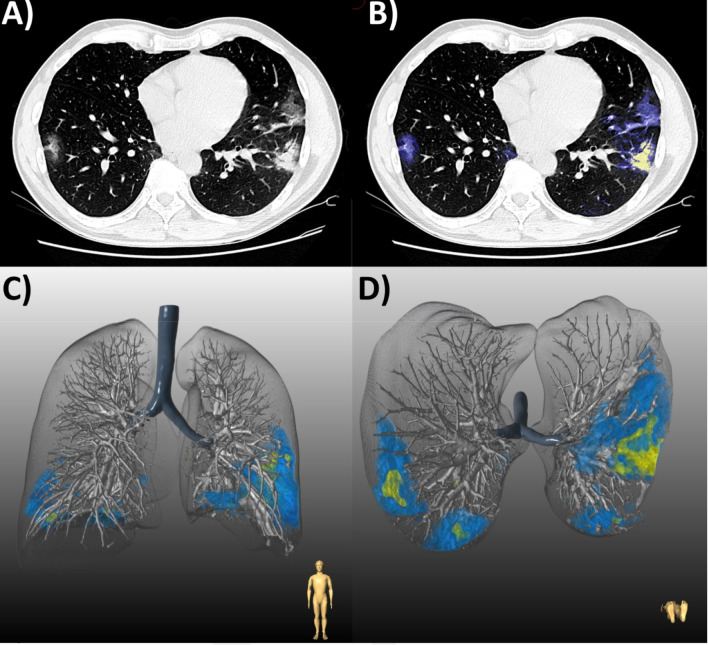
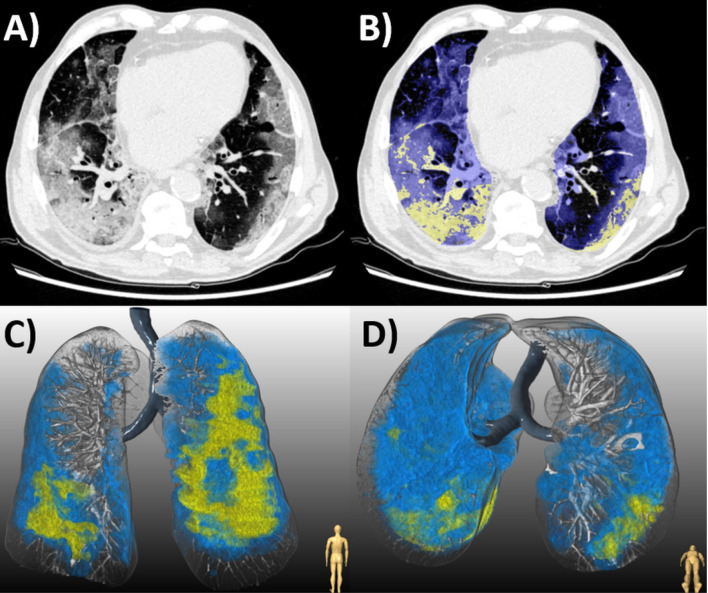
This was a retrospective analysis of a prospective international registry of consecutive patients with laboratory-confirmed COVID-19 and chest CT imaging, admitted to four centers between January 10 and May 6, 2020. Total burden (expressed as a percentage) and mean attenuation of ground glass opacities (GGO) and consolidation were quantified from CT using semi-automated research software. The primary outcome was clinical deterioration (intensive care unit admission, invasive mechanical ventilation, or vasopressor therapy) or in-hospital death. Logistic regression was performed to assess the predictive value of clinical and CT parameters for the primary outcome.
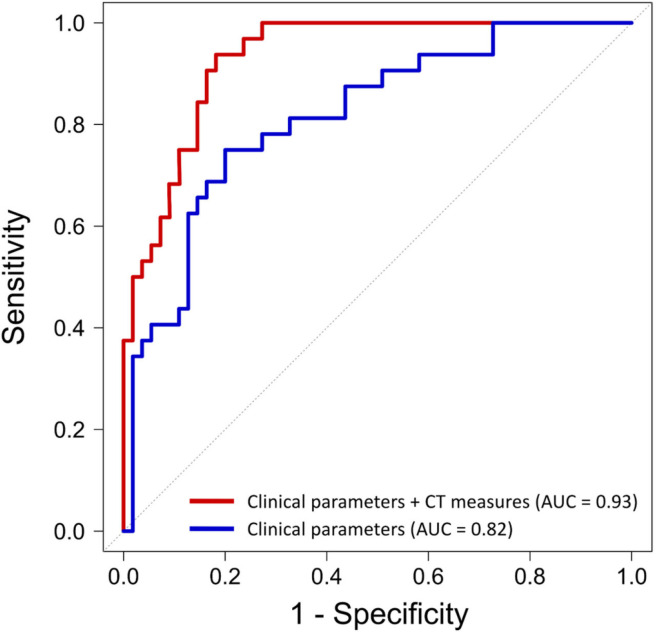
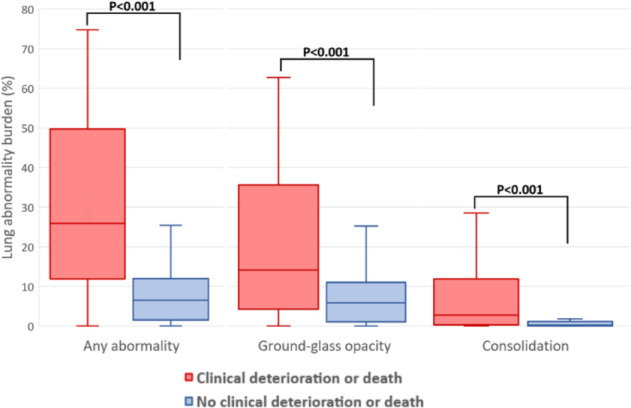
The final population comprised 120 patients (mean age 64 ± 16 years, 78 men), of whom 39 (32.5%) experienced clinical deterioration or death. In multivariable regression of clinical and CT parameters, consolidation burden (odds ratio [OR], 3.4; 95% confidence interval [CI]: 1.7, 6.9 per doubling; = .001) and increasing GGO attenuation (OR, 3.2; 95% CI: 1.3, 8.3 per standard deviation, = .02) were independent predictors of deterioration or death; as was C-reactive protein (OR, 2.1; 95% CI: 1.3, 3.4 per doubling; = .004), history of heart failure (OR 1.3; 95% CI: 1.1, 1.6, = .01), and chronic lung disease (OR, 1.3; 95% CI: 1.0, 1.6; = .02). Quantitative CT measures added incremental predictive value beyond a model with only clinical parameters (area under the curve, 0.93 vs 0.82, = .006). The optimal prognostic cutoffs for burden of COVID-19 pneumonia as determined by Youden's index were consolidation of greater than or equal to 1.8% and GGO of greater than or equal to 13.5%.
Quantitative burden of consolidation or GGO on chest CT independently predict clinical deterioration or death in patients with COVID-19 pneumonia. CT-derived measures have incremental prognostic value over and above clinical parameters, and may be useful for risk stratifying patients with COVID-19.
探讨CT衍生的新型冠状病毒肺炎定量负担和衰减对预测临床恶化或死亡的独立及增量价值。
这是一项对2020年1月10日至5月6日期间入住四个中心的连续实验室确诊新型冠状病毒肺炎且有胸部CT影像的患者进行的前瞻性国际登记研究的回顾性分析。使用半自动研究软件从CT中量化总负担(以百分比表示)以及磨玻璃影(GGO)和实变的平均衰减。主要结局为临床恶化(入住重症监护病房、有创机械通气或血管活性药物治疗)或院内死亡。进行逻辑回归以评估临床和CT参数对主要结局的预测价值。
最终纳入120例患者(平均年龄64±16岁,男性78例),其中39例(32.5%)出现临床恶化或死亡。在临床和CT参数的多变量回归中,实变负担(比值比[OR],3.4;95%置信区间[CI]:每增加一倍为1.7,6.9;P = 0.001)和GGO衰减增加(OR,3.2;95%CI:每标准差为1.3,8.3;P = 0.02)是恶化或死亡的独立预测因素;C反应蛋白(OR,2.1;95%CI:每增加一倍为1.3,3.4;P = 0.004)、心力衰竭病史(OR 1.3;95%CI:1.1,1.6;P = 0.01)和慢性肺病(OR,1.3;95%CI:1.0,1.6;P = 0.02)也是如此。定量CT测量在仅包含临床参数的模型之外增加了增量预测价值(曲线下面积,0.93对vs0.82;P = 0.006)。根据约登指数确定的新型冠状病毒肺炎负担的最佳预后临界值为实变大于或等于1.8%和GGO大于或等于13.5%。
胸部CT上实变或GGO的定量负担可独立预测新型冠状病毒肺炎患者的临床恶化或死亡。CT衍生的测量在临床参数之外具有增量预后价值,可能有助于对新型冠状病毒肺炎患者进行风险分层。