Monroy-Iglesias Maria J, Tagliabue Marta, Dickinson Harvey, Roberts Graham, De Berardinis Rita, Russell Beth, Moss Charlotte, Irwin Sophie, Olsburgh Jonathon, Cocco Ivana Maria Francesca, Schizas Alexis, McCrindle Sarah, Nath Rahul, Brunet Aina, Simo Ricard, Tornari Chrysostomos, Srinivasan Parthi, Prachalias Andreas, Davies Andrew, Geh Jenny, Fraser Stephanie, Routledge Tom, Ma RuJun, Doerge Ella, Challacombe Ben, Nair Raj, Hadjipavlou Marios, Scarpinata Rosaria, Sorelli Paolo, Dolly Saoirse, Mistretta Francesco Alessandro, Musi Gennaro, Casiraghi Monica, Aloisi Alessia, Dell'Acqua Andrea, Scaglione Donatella, Zanoni Stefania, Rampazio Da Silva Daniele, Brambilla Daniela, Bertolotti Raffaella, Peruzzotti Giulia, Maggioni Angelo, de Cobelli Ottavio, Spaggiari Lorenzo, Ansarin Mohssen, Mastrilli Fabrizio, Gandini Sara, Jain Urvashi, Hamed Hisham, Haire Kate, Van Hemelrijck Mieke
Faculty of Life Sciences and Medicine, Translational Oncology & Urology Research (TOUR), King's College London, London WC2R 2LS, UK.
Division of Otolaryngology and Head and Neck Surgery, European Institute of Oncology IRCCS, 20122 Milan, Italy.
Cancers (Basel). 2021 Mar 30;13(7):1597. doi: 10.3390/cancers13071597.
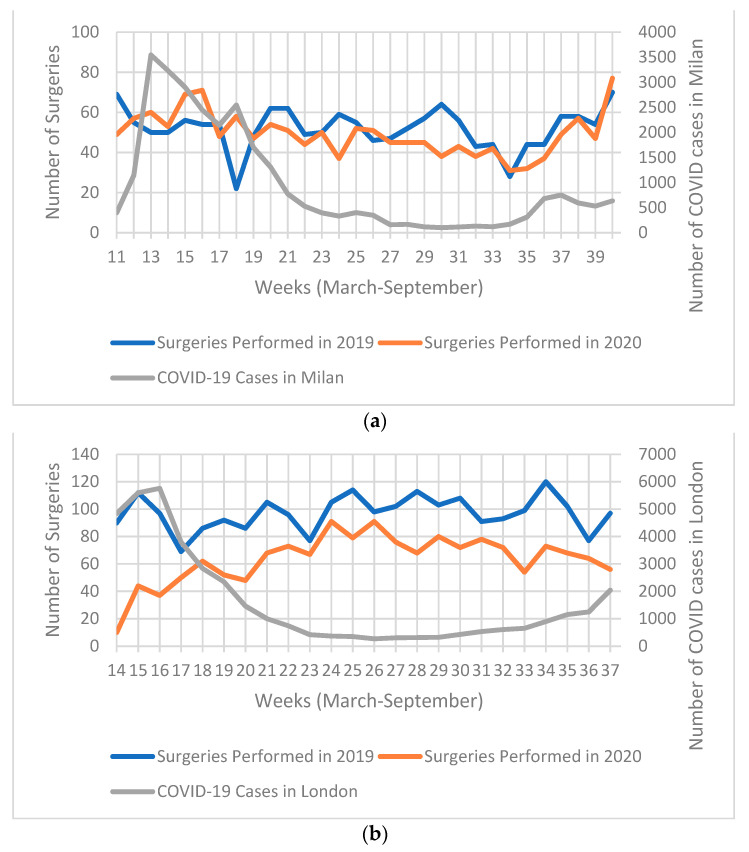
The SARS-CoV-2 (COVID-19) pandemic is having a large effect on the management of cancer patients. This study reports on the approach and outcomes of cancer patients receiving radical surgery with curative intent between March and September 2020 (in comparison to 2019) in the European Institute of Oncology, IRCCS (IEO) in Milan and the South East London Cancer Alliance (SELCA). Both institutions implemented a COVID-19 minimal pathway where patients were required to self-isolate prior to admission and were swabbed for COVID-19 within 72 h of surgery. Positive patients had surgery deferred until a negative swab. At IEO, radical surgeries declined by 6% as compared to the same period in 2019 ( = 1477 vs. 1560, respectively). Readmissions were required for 3% ( = 41), and <1% ( = 9) developed COVID-19, of which only one had severe disease and died. At SELCA, radical surgeries declined by 34% ( = 1553 vs. 2336). Readmissions were required for 11% ( = 36), <1% ( = 7) developed COVID-19, and none died from it. Whilst a decline in number of surgeries was observed in both centres, the implemented COVID-19 minimal pathways have shown to be safe for cancer patients requiring radical treatment, with limited complications and almost no COVID-19 infections.
严重急性呼吸综合征冠状病毒2(SARS-CoV-2,即新冠病毒)大流行对癌症患者的管理产生了重大影响。本研究报告了2020年3月至9月期间(与2019年相比),米兰欧洲肿瘤研究所(IRCCS,IEO)和伦敦东南部癌症联盟(SELCA)接受根治性手术且有治愈意图的癌症患者的治疗方法及结果。两家机构都实施了新冠病毒最小化路径,要求患者在入院前进行自我隔离,并在手术72小时内进行新冠病毒检测。检测呈阳性的患者手术推迟至检测结果为阴性。在IEO,与2019年同期相比,根治性手术减少了6%(分别为1477例和1560例)。3%(41例)患者需要再次入院,<1%(9例)患者感染了新冠病毒,其中只有1例病情严重并死亡。在SELCA,根治性手术减少了34%(1553例和2336例)。11%(36例)患者需要再次入院,<1%(7例)患者感染了新冠病毒,且无人因此死亡。虽然两个中心的手术数量均有所下降,但实施的新冠病毒最小化路径已证明对需要根治性治疗的癌症患者是安全的,并发症有限,几乎没有新冠病毒感染。