Department of Genetics and Genomics, Icahn School of Medicine at Mount Sinai, New York, New York; Icahn Institute for Data Science and Genomic Technology, New York, New York.
Hematology and Medical Oncology, Icahn School of Medicine at Mount Sinai, New York, New York; Human Immune Monitoring Center, Icahn School of Medicine at Mount Sinai, New York, New York.
Cell Mol Gastroenterol Hepatol. 2021;12(2):599-632. doi: 10.1016/j.jcmgh.2021.03.012. Epub 2021 Apr 2.
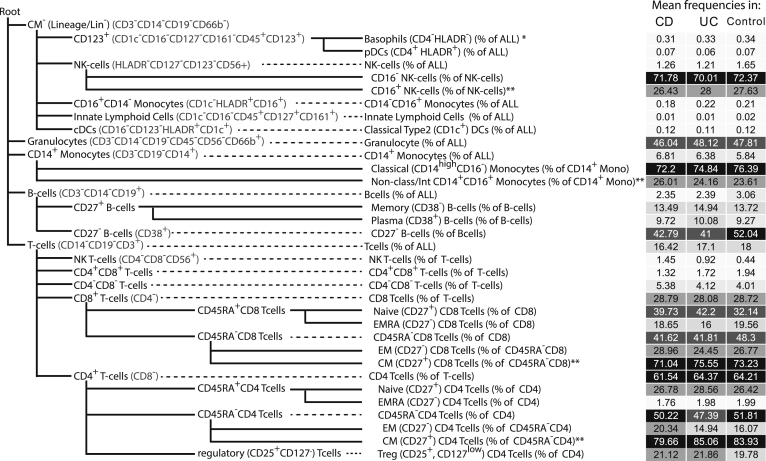
Inflammatory bowel disease (IBD) is a complex disease with variable presentation, progression, and response to therapies. Current disease classification is based on subjective clinical phenotypes. The peripheral blood immunophenome can reflect local inflammation, and thus we measured 39 circulating immune cell types in a large cohort of IBD and control subjects and performed immunotype:phenotype associations.
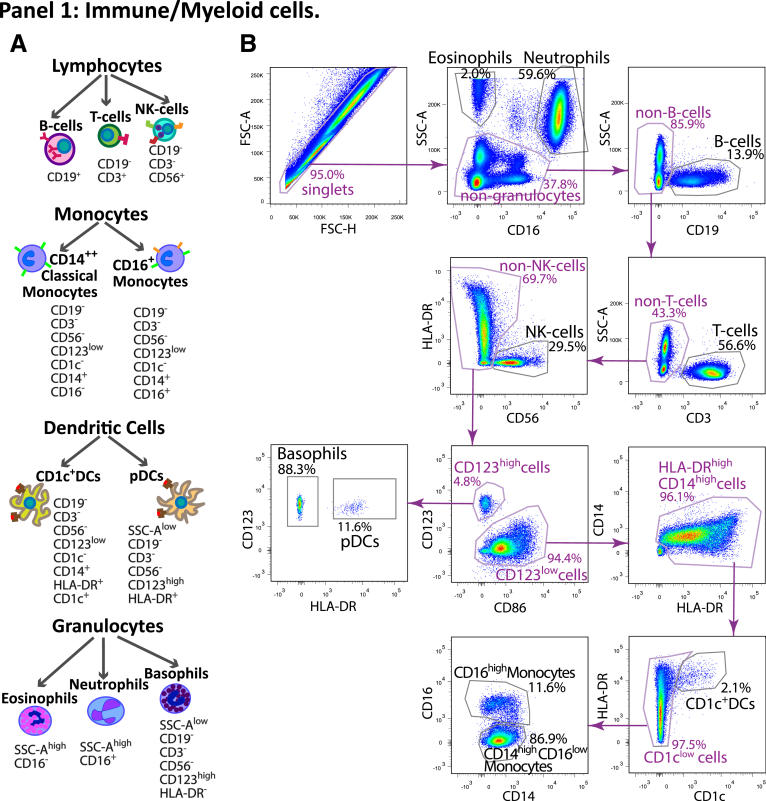
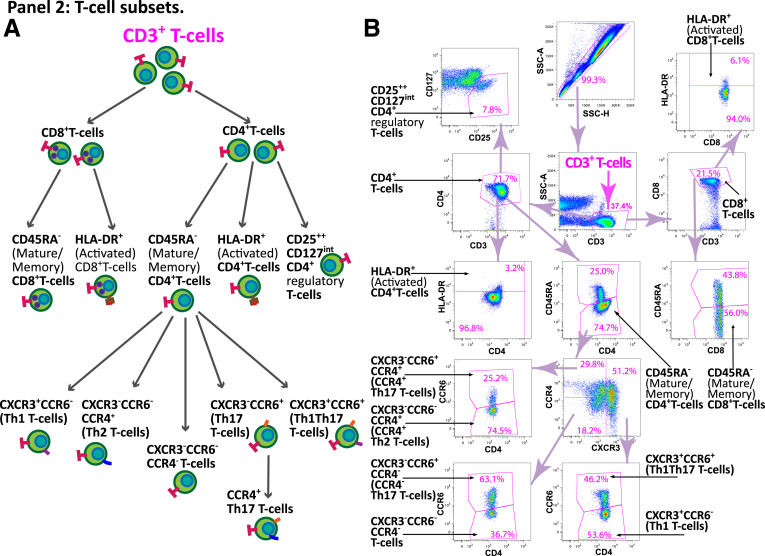
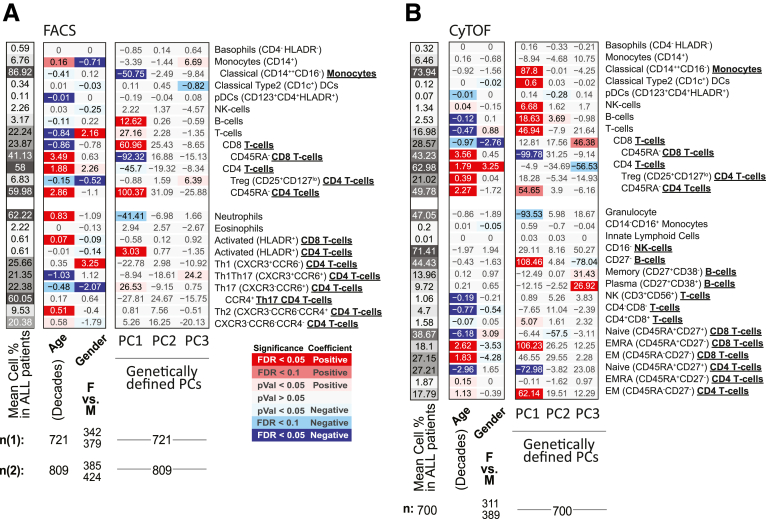
We performed fluorescence-activated cell sorting or CyTOF analysis on blood from 728 Crohn's disease, 464 ulcerative colitis, and 334 non-IBD patients, with available demographics, endoscopic and clinical examinations and medication use.
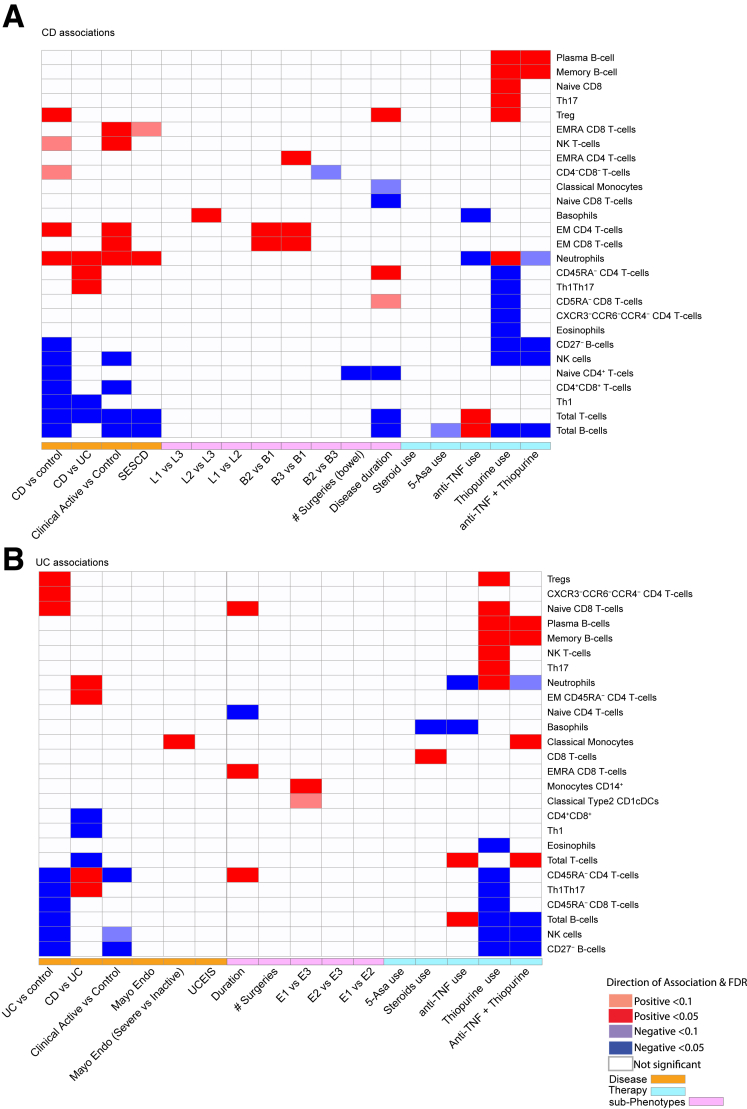
We observed few immune cell types commonly affected in IBD (lowered natural killer cells, B cells, and CD45RA CD8 T cells). Generally, the immunophenome was distinct between ulcerative colitis and Crohn's disease. Within disease subtype, there were further distinctions, with specific immune cell types associating with disease duration, behavior, and location. Thiopurine monotherapy altered abundance of many cell types, often in the same direction as disease association, while anti-tumor necrosis factor (anti-TNF) monotherapy demonstrated an opposing pattern. Concomitant use of an anti-TNF and thiopurine was not synergistic, but rather was additive. For example, thiopurine monotherapy use alone or in combination with anti-TNF was associated with a dramatic reduction in major subclasses of B cells.
We present a peripheral map of immune cell changes in IBD related to disease entity and therapies as a resource for hypothesis generation. We propose the changes in B cell subsets could affect antibody formation and potentially explain the mechanism behind the superiority of combination therapy through the impact of thiopurines on pharmacokinetics of anti-TNFs.
炎症性肠病(IBD)是一种具有多变临床表现、进展和治疗反应的复杂疾病。目前的疾病分类基于主观的临床表型。外周血免疫表型可以反映局部炎症,因此我们在一个大型 IBD 和对照受试者队列中测量了 39 种循环免疫细胞类型,并进行了免疫表型:表型关联分析。
我们对 728 例克罗恩病、464 例溃疡性结肠炎和 334 例非 IBD 患者的血液进行了荧光激活细胞分选或 CyTOF 分析,这些患者有可用的人口统计学、内镜和临床检查以及药物使用数据。
我们观察到在 IBD 中很少有共同受影响的免疫细胞类型(自然杀伤细胞、B 细胞和 CD45RA CD8 T 细胞减少)。通常,溃疡性结肠炎和克罗恩病之间的免疫表型存在明显差异。在疾病亚型内,还有进一步的区别,特定的免疫细胞类型与疾病持续时间、行为和位置有关。硫唑嘌呤单药治疗改变了许多细胞类型的丰度,通常与疾病关联的方向相同,而抗肿瘤坏死因子(anti-TNF)单药治疗则表现出相反的模式。抗 TNF 和硫唑嘌呤的联合使用不是协同的,而是相加的。例如,硫唑嘌呤单药治疗或与抗 TNF 联合使用与 B 细胞主要亚群的显著减少有关。
我们提供了 IBD 相关免疫细胞变化的外周图谱,与疾病实体和治疗相关,作为产生假说的资源。我们提出 B 细胞亚群的变化可能会影响抗体的形成,并可能通过硫唑嘌呤对 anti-TNFs 的药代动力学的影响来解释联合治疗的优越性的机制。