Department of Medical Sciences, Uppsala University, Uppsala, Sweden.
Department of Medical Sciences and Uppsala Clinical Research Center, Uppsala University, Uppsala, Sweden.
PLoS One. 2021 Apr 8;16(4):e0249830. doi: 10.1371/journal.pone.0249830. eCollection 2021.
Sex-differences in the pathobiology of myocardial infarction are well established but incompletely understood. Improved knowledge on this topic may help clinicians to improve management of men and women with myocardial infarction.
In this registry-based cohort study (SWEDEHEART), we analyzed 175 circulating biomarkers reflecting various pathobiological axes in 856 men and 243 women admitted to Swedish coronary care units because of myocardial infarction. Two multimarker panels were applied (Proximity Extension Assay [Olink Bioscience], Multiple Reaction Monitoring mass spectrometry). Lasso analysis (penalized logistic regression), multiple testing-corrected Mann-Whitney tests and Cox regressions were used to assess sex-differences in the concentrations of these biomarkers and their implications on all-cause mortality and major adverse events (median follow-up up to 6.6 years).
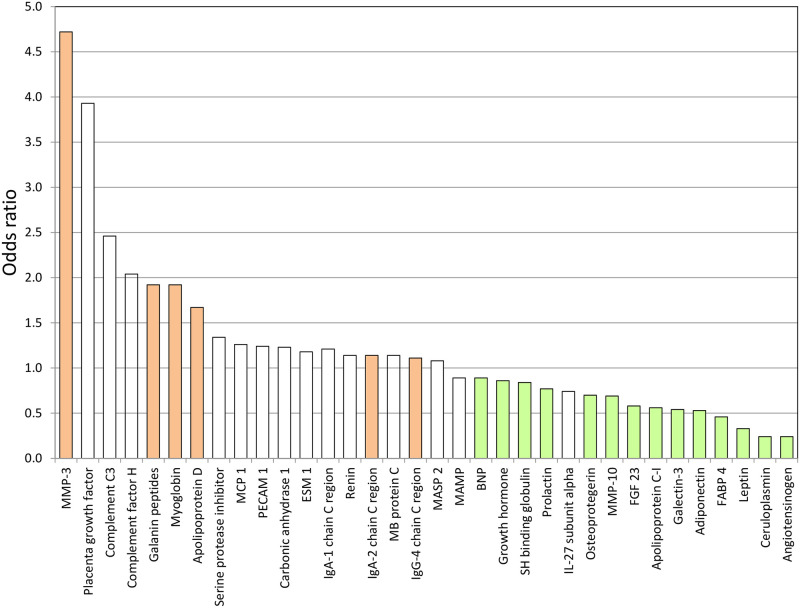
Biomarkers provided a very high discrimination between both sexes, when considered simultaneously (c-statistics 0.972). Compared to women, men had higher concentrations of six biomarkers with the most pronounced differences seen for those reflecting atherogenesis, myocardial necrosis and metabolism. Women had higher concentrations of 14 biomarkers with the most pronounced differences seen for those reflecting activation of the renin-angiotensin-aldosterone axis, inflammation and for adipokines. There were no major variations between sexes in the associations of these biomarkers with outcome.
Severable sex-differences exist in the expression of biomarkers in patients with myocardial infarction. While these differences had no impact on outcome, our data suggest the presence of various sex-related pathways involved in the development of coronary atherosclerosis, the progression to plaque rupture and acute myocardial damage, with a greater heterogeneity in women.
心肌梗死的病理生物学存在性别差异,这已得到充分证实,但仍不完全清楚。在这一领域的知识进步可以帮助临床医生改善对心肌梗死男性和女性患者的管理。
在这项基于登记的队列研究(SWEDEHEART)中,我们分析了 856 名男性和 243 名因心肌梗死入住瑞典冠状动脉护理病房的患者的 175 种循环生物标志物,这些生物标志物反映了各种病理生物学轴。应用了两种多标志物检测试剂盒(临近延伸分析[Olink Bioscience]、多重反应监测质谱法)。采用套索分析(惩罚逻辑回归)、多重检验校正的曼-惠特尼检验和 Cox 回归分析来评估这些生物标志物的浓度在性别之间的差异,以及它们对全因死亡率和主要不良事件(中位数随访时间长达 6.6 年)的影响。
当同时考虑这些生物标志物时,它们在两性之间具有非常高的区分能力(c 统计量为 0.972)。与女性相比,男性的 6 种生物标志物浓度更高,其中反映动脉粥样硬化、心肌坏死和代谢的标志物差异最为显著。女性的 14 种生物标志物浓度更高,其中反映肾素-血管紧张素-醛固酮轴激活、炎症和脂肪因子的标志物差异最为显著。这些生物标志物与结局的关联在性别之间没有明显差异。
在心肌梗死患者中,生物标志物的表达存在可衡量的性别差异。尽管这些差异对结局没有影响,但我们的数据表明,存在与冠状动脉粥样硬化发展、斑块破裂和急性心肌损伤相关的各种性别相关途径,女性的异质性更大。