Center for Fundamental Living Technology (FLinT) Department for Physics, Chemistry and Pharmacy, University of Southern Denmark, Odense, Denmark.
Santa Fe Institute, Santa Fe, New Mexico, United States of America.
PLoS One. 2021 Apr 9;16(4):e0249733. doi: 10.1371/journal.pone.0249733. eCollection 2021.
Initially, the relative sizes of the asymptomatic and the symptomatic infected populations were not known for the COVID-19 pandemic and neither was the actual fatality rate. Therefore it was not clear either how the pandemic would impact the healthcare system. As a result it was initially predicted that the COVID-19 epidemic in Denmark would overwhelm the healthcare system and thus both the diagnosis and treatment of other hospital patients were compromised for an extended period.
To develop a mathematical model, which includes both asymptomatic and symptomatic infected persons, for early estimation of the epidemic's course, its Infection Fatality Rate and the healthcare system load in Denmark, both retrospectively and prospectively.
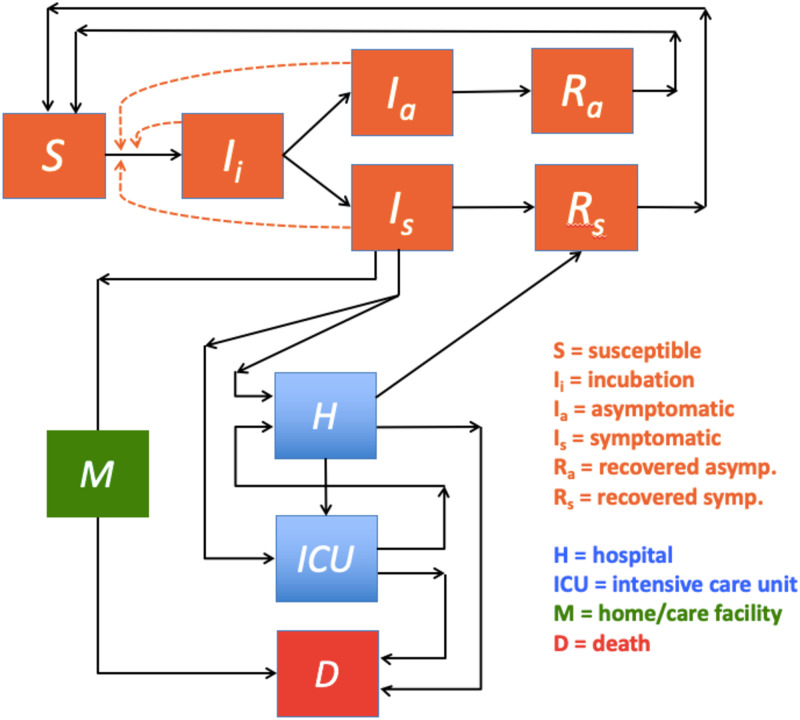
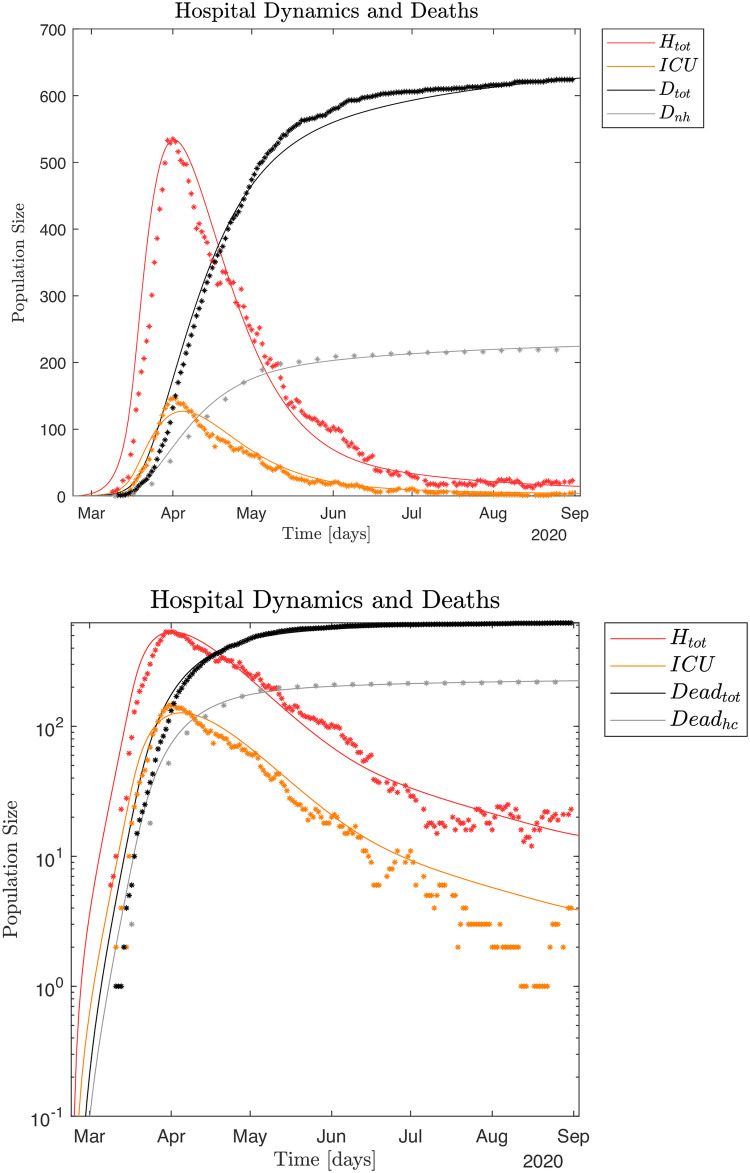
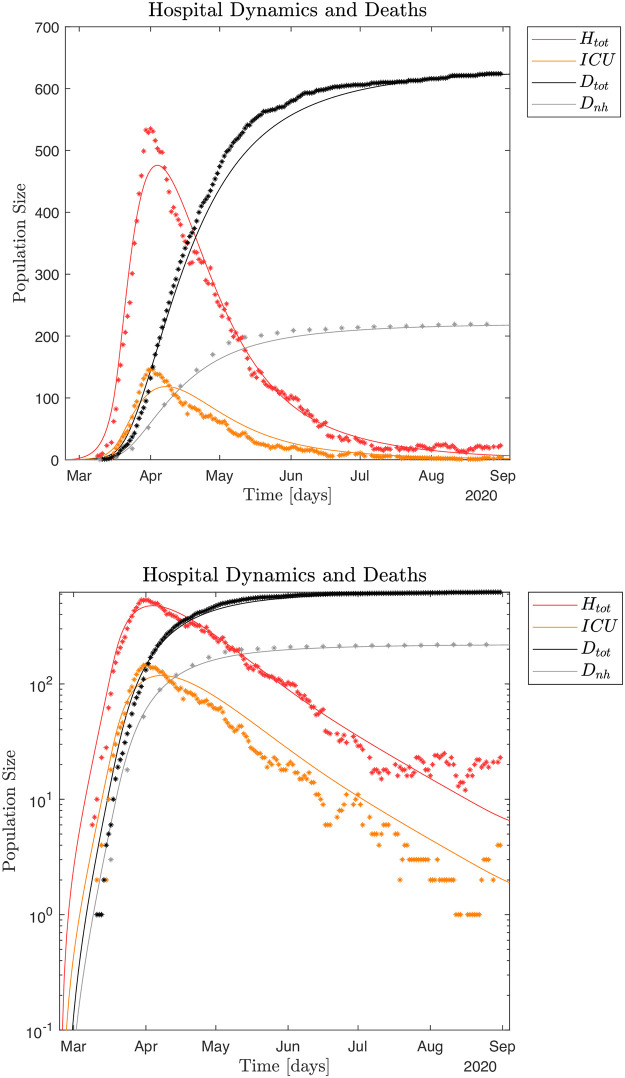
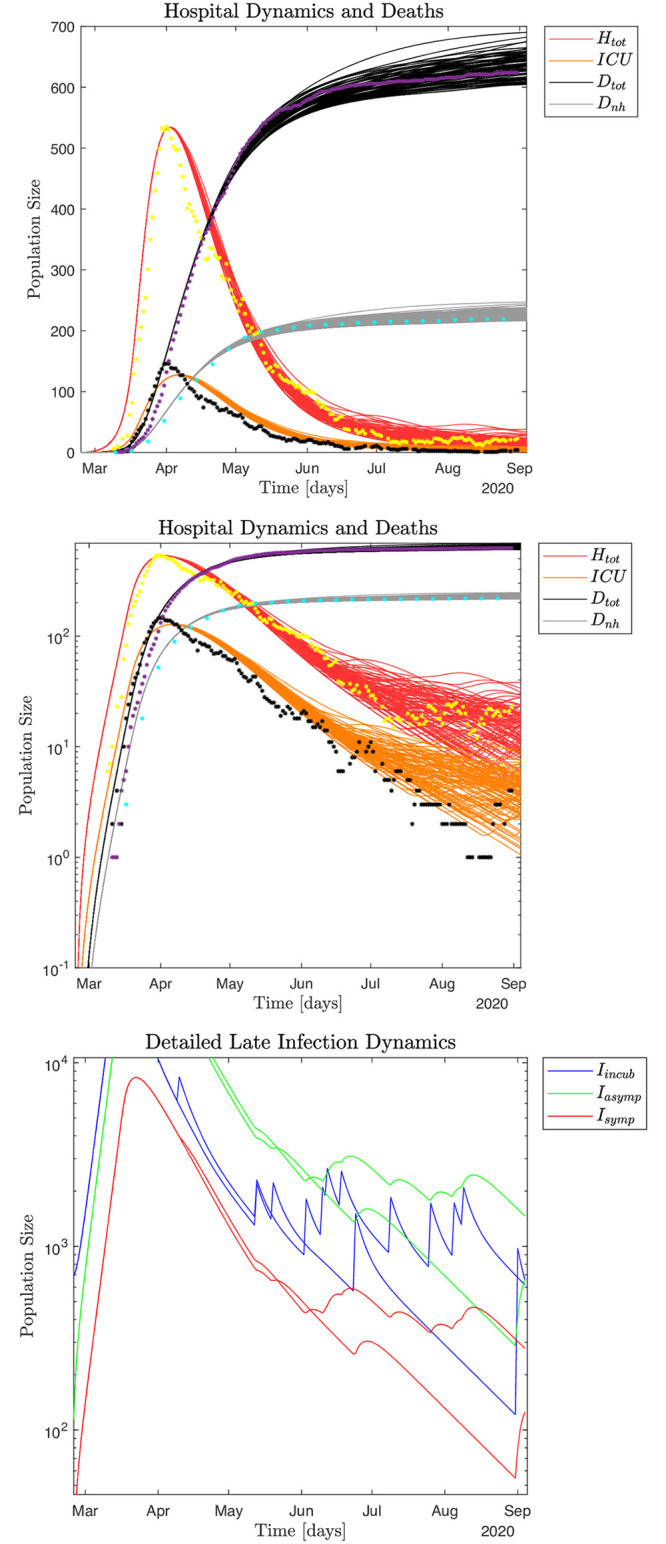
The SEIRS (Susceptible-Exposed-Infected-Recovered-Susceptible) model including deaths outside hospitals and separate assessments of symptomatic and asymptomatic cases (based on seroprevalence) with different immunological memories. Optimal model parameters are in part identified by Monte Carlo based Least Square Error methods while micro-outbreaks are modeled by noise and explored in Monte Carlo simulations. Estimates for infected population sizes are obtained by using a quasi steady state method.
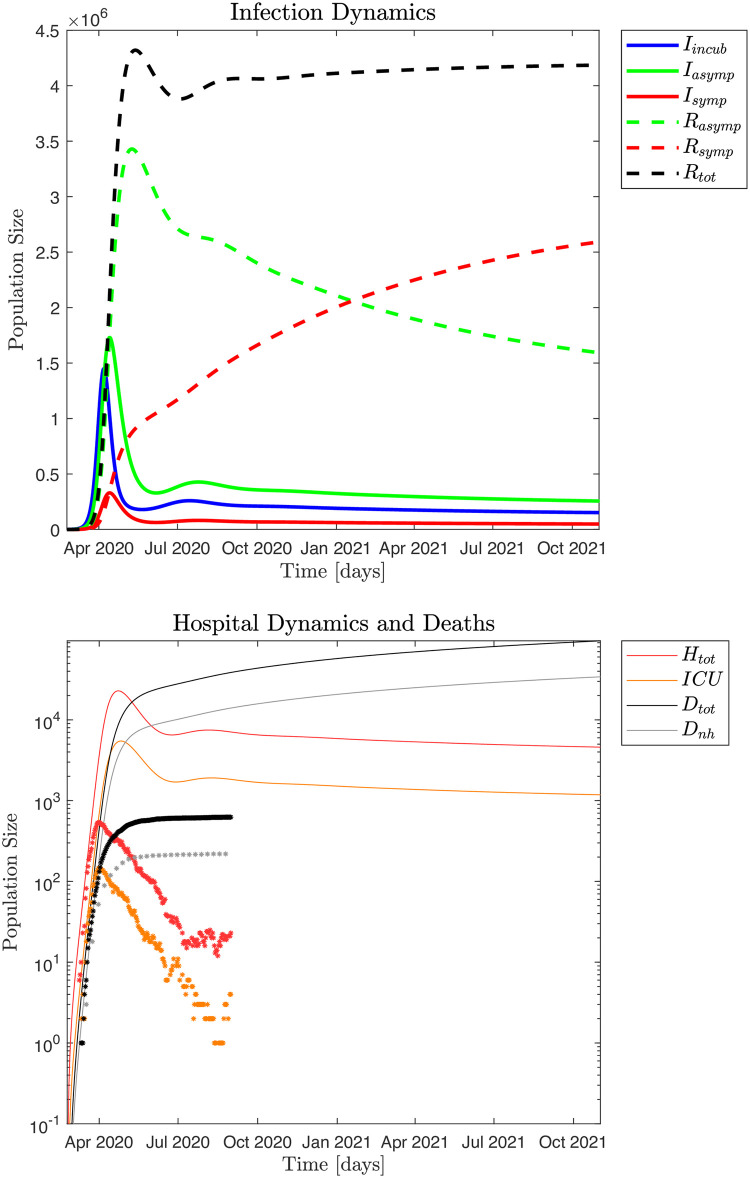
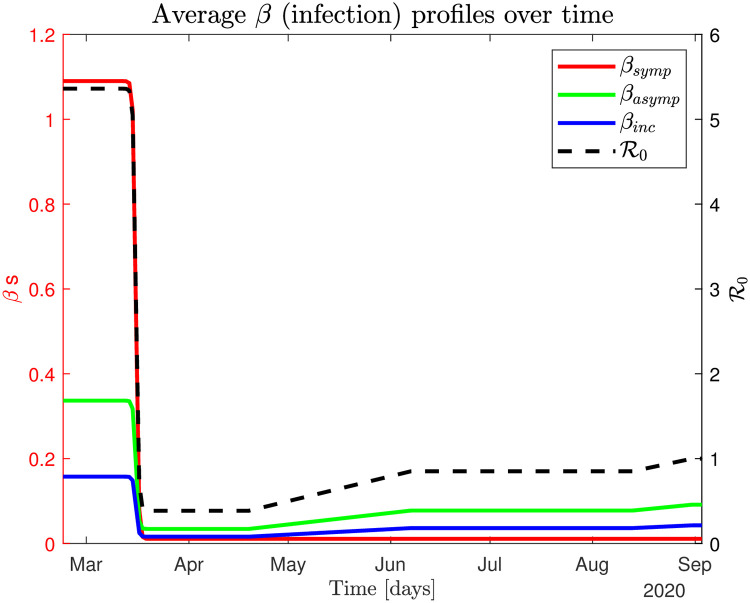
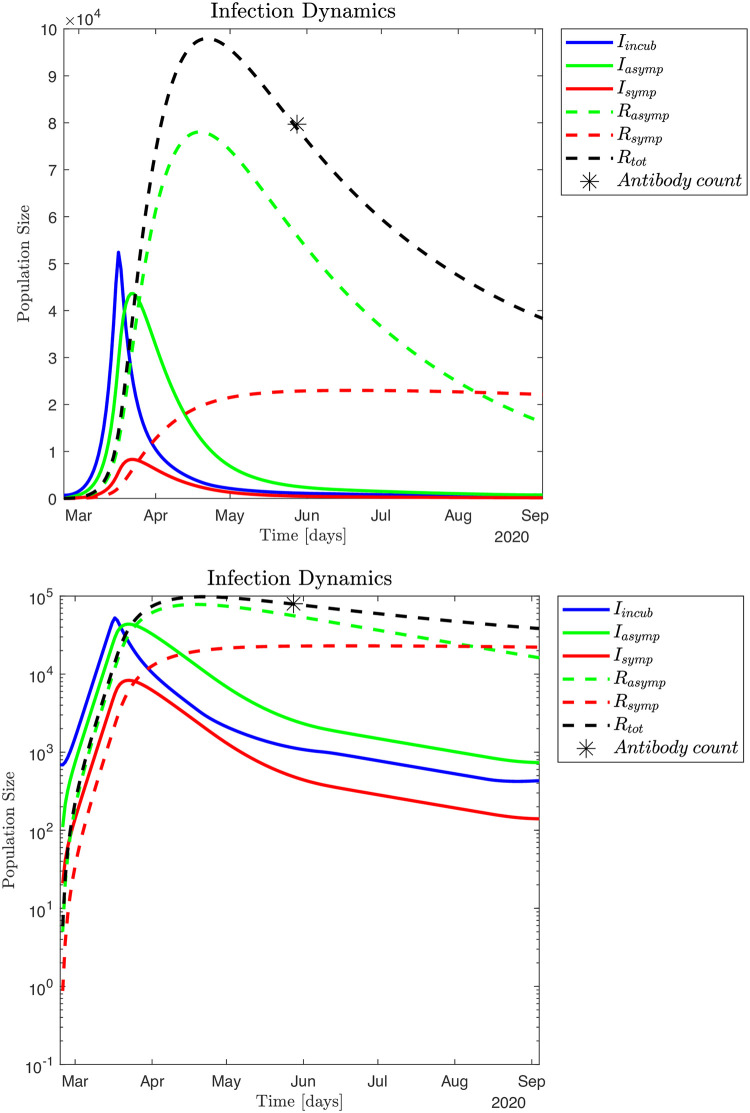
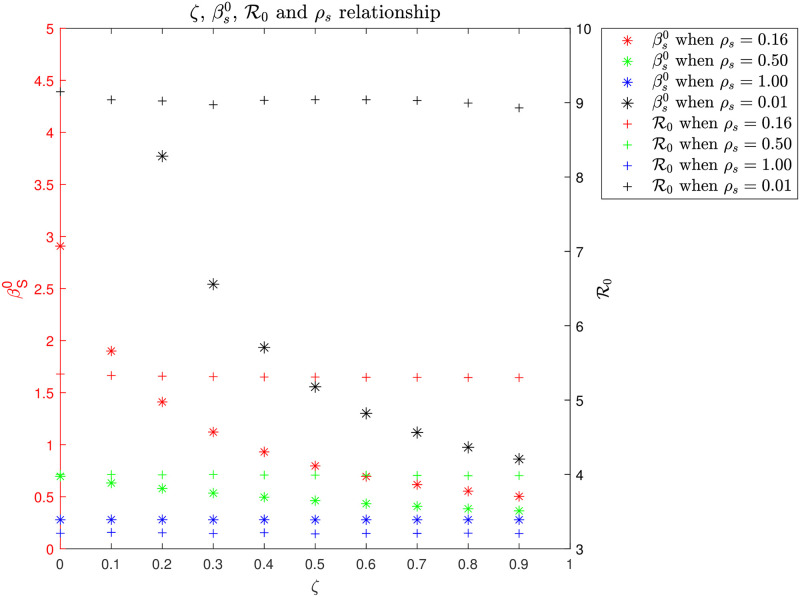
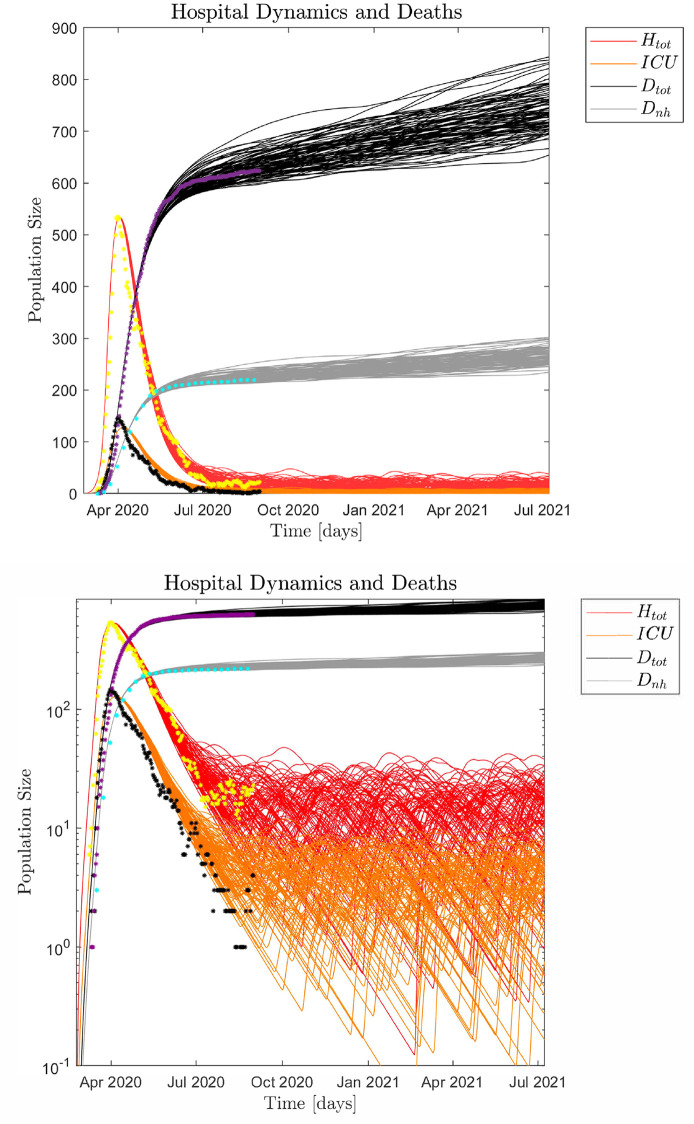
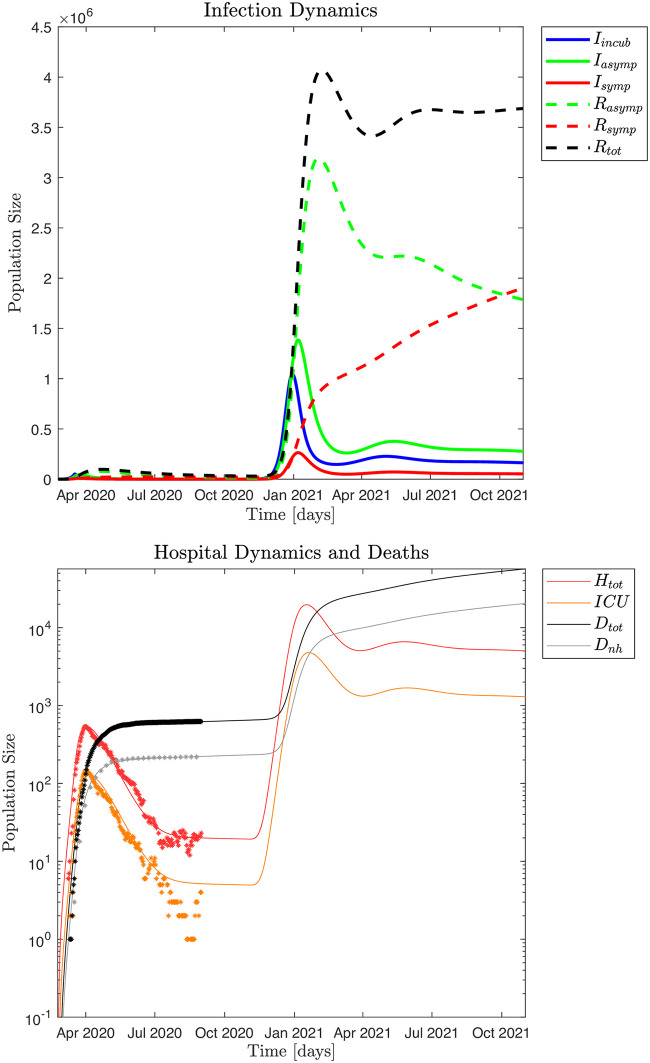
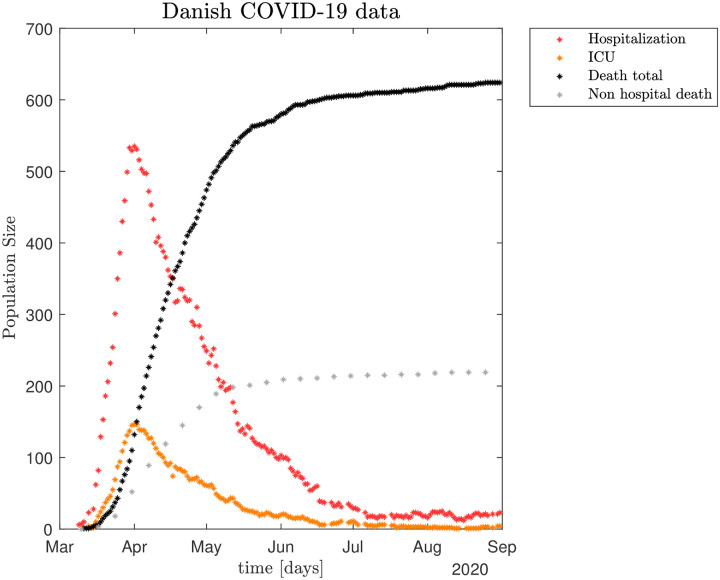
The calculations and simulations made by the model were shown to fit with the observed development of the COVID-19 epidemic in Denmark. The antibody prevalence in the general population in May 2020 was 1.37%, which yields a relative frequency of symptomatic and asymptomatic cases of 1 to 5.2. Due to the large asymptomatic population, the Infection Mortality Rate was only 0.4%. However, with no non-pharmacological restrictions the COVID-19 death toll was calculated to have more than doubled the national average yearly deaths within a year. The transmission rate ℜ0 was 5.4 in the initial free epidemic period, 0.4 in the lock-down period and 0.8-1.0 in the successive re-opening periods through August 2020. The large asymptomatic population made the termination of the epidemic difficult and micro-outbreaks occurred when the country re-opened. The estimated infected population size July 15 to August 15 was 2,100 and 12,200 for October 1-20, 2020.
The results of the model show, that COVID-19 has a low Infection Fatality Rate because the majority of infected persons are either asymptomatic or with few symptoms. A minority of the infected persons, therefore, requires hospitalization. That means that for a given infection pressure of both symptomatic and asymptomatic infected there will be a lower pressure on the capacity of the health care system than previously predicted. Further the epidemic will be difficult to terminate since about 84% of the infected individuals are asymptomatic but still contagious. The model may be useful if a major infection wave occurs in the autumn-winter season as it could make robust estimates both for the scale of an ongoing expanding epidemic and for the expected load on the healthcare system. The simulation may also be useful to evaluate different testing strategies based on estimated infected population sizes. The model can be adjusted and scaled to other regions and countries, which is illustrated with Spain and USA.
最初,对于 COVID-19 大流行,我们并不知道无症状和有症状感染者的相对规模,也不知道实际死亡率。因此,我们也不清楚大流行将如何影响医疗保健系统。因此,最初预测 COVID-19 疫情在丹麦将使医疗保健系统不堪重负,从而在很长一段时间内影响对其他住院患者的诊断和治疗。
开发一种数学模型,该模型包括无症状和有症状感染者,用于早期估计丹麦的疫情进程、其感染死亡率和医疗保健系统负荷,包括回顾性和前瞻性估计。
SEIRS(易感-暴露-感染-恢复-易感)模型包括医院外死亡,并对基于血清流行率的有症状和无症状病例(基于血清流行率)进行单独评估,具有不同的免疫记忆。通过基于蒙特卡罗的最小二乘误差方法部分确定最佳模型参数,而微爆发则通过噪声建模,并在蒙特卡罗模拟中进行探索。通过准稳态方法获得感染人群规模的估计。
模型的计算和模拟结果表明,它与丹麦 COVID-19 疫情的实际发展情况相符。2020 年 5 月,普通人群中的抗体流行率为 1.37%,这意味着有症状和无症状病例的相对频率为 1 比 5.2。由于无症状人群庞大,感染死亡率仅为 0.4%。然而,由于没有非药物限制,COVID-19 的死亡人数预计将在一年内超过全国平均年死亡人数的两倍。在最初的自由流行期间,传播率 ℜ0 为 5.4,封锁期间为 0.4,2020 年 8 月至 8 月连续重新开放期间为 0.8-1.0。大量的无症状人群使疫情难以结束,当该国重新开放时会发生微爆发。2020 年 7 月 15 日至 8 月 15 日和 10 月 1 日至 20 日的估计感染人群规模分别为 2100 和 12200。
模型结果表明,COVID-19 的感染死亡率较低,因为大多数感染者要么无症状,要么症状很少。因此,少数感染者需要住院治疗。这意味着,对于有症状和无症状感染者的给定感染压力,医疗保健系统的压力将低于先前的预测。此外,由于大约 84%的感染者无症状但仍具有传染性,因此疫情将难以结束。如果秋季-冬季出现大规模感染浪潮,该模型可能会很有用,因为它可以对正在进行的不断扩大的疫情规模以及对医疗保健系统的预期负荷进行强有力的估计。该模拟还可以用于评估基于估计的感染人群规模的不同测试策略。该模型可以调整和扩展到其他地区和国家,西班牙和美国的情况就是如此。