Adamkiewicz Mateusz, Bryniarski Piotr, Kowalik Maksymilian, Burzyński Bartłomiej, Rajwa Paweł, Paradysz Andrzej
Department of Urology, Medical University of Silesia, Zabrze, Poland.
Department of Rehabilitation, Faculty of Health Sciences, Medical University of Silesia, Katowice, Poland.
Front Oncol. 2021 Mar 26;11:655000. doi: 10.3389/fonc.2021.655000. eCollection 2021.
Transurethral resection of bladder tumor with subsequent BCG immunotherapy is the current gold standard in the treatment of high risk and some medium-risk non-muscle invasive bladder cancer. Clinical factors like stage, grade, age and gender are well-know predictors of progression to muscle-invasive bladder cancer. In recent years novel hematological biomarkers were shown to be independent predictors of progression. This study aimed to evaluate which of these novel markers has the highest prognostic value of progression in patients with bladder cancer receiving BCG immunotherapy.
We retrospectively analyzed the data of 125 patients with non-muscle invasive bladder cancer who received BCG immunotherapy. Of these, 61 progressed to muscle-invasive disease or had high-grade recurrence. These patients were compared with the group who did not progress (n = 64). Clinical data including stage, grade, age, gender, smoking status and observational time was collected. Besides, information on blood count analysis was obtained from ambulatory digital charts. On this basis neutrophil-to-lymphocyte ratio (NLR), platelet-to lymphocyte ratio (PLR) and lymphocyte-to-monocyte ratio (LMR) was counted and compared between groups.
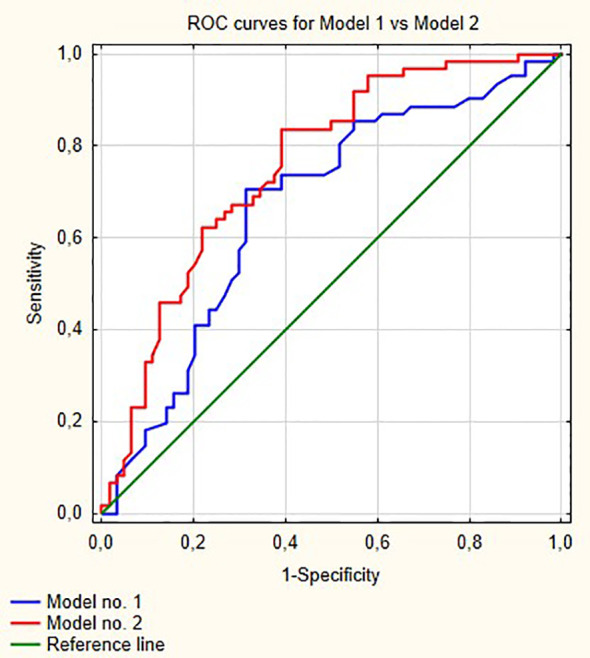
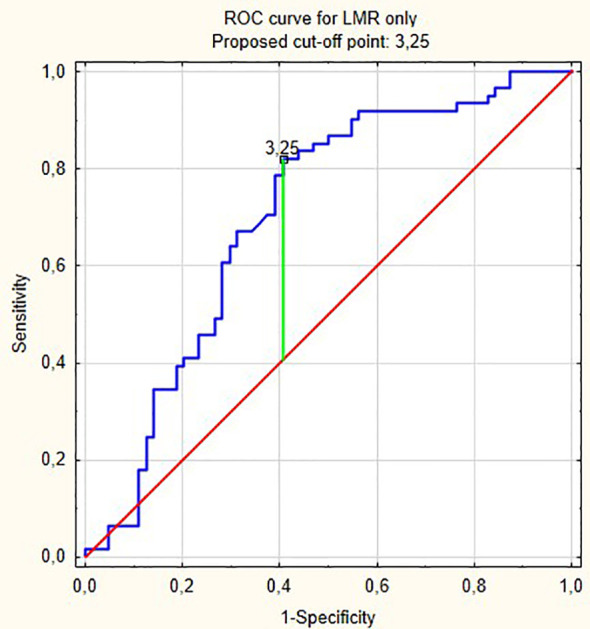
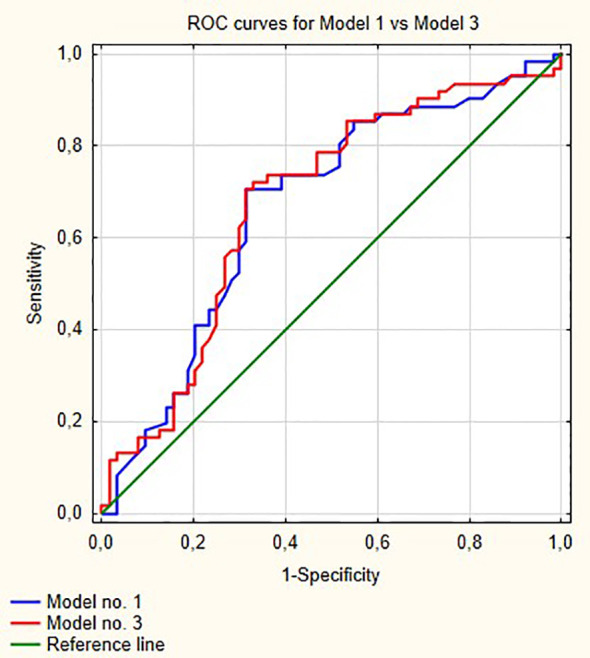
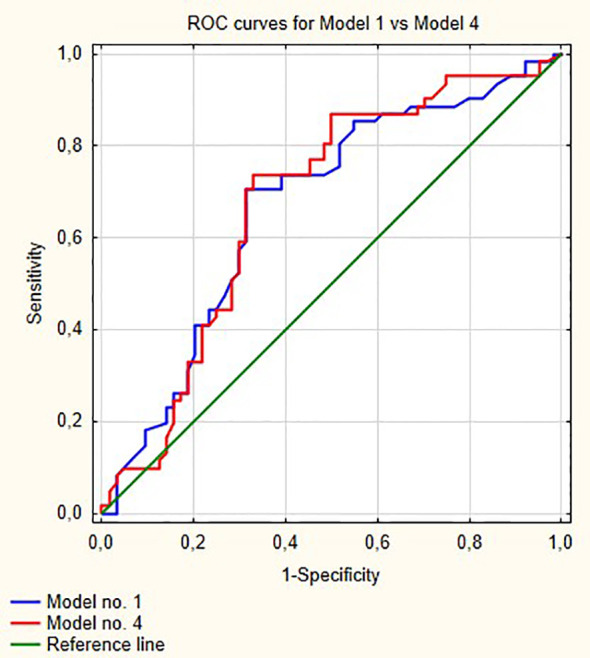
NLR, PLR and LMR were shown to be independent prognostic markers of progression in multivariable analysis. The model with stage, grade, age, gender, smoking status and LMR had the highest prognostic values of all models (area under curve [AUC] = 0.756). The cut-off point according to ROC curves for LMR was 3.25. Adding LMR to the baseline model including clinical variables significantly increased area under curve by 0.08 (p = 0.001). NLR and PLR did not increase areas under curve significantly to baseline model.
LMR outperformed NLR and PLR for prediction of progression in patients with non-muscle-invasive bladder cancer receiving BCG immunotherapy. LMR, as an easily obtainable biomarker, should be incorporated to the present risk stratification models.
经尿道膀胱肿瘤切除术联合后续卡介苗免疫治疗是目前治疗高危及部分中危非肌层浸润性膀胱癌的金标准。临床因素如分期、分级、年龄和性别是进展为肌层浸润性膀胱癌的众所周知的预测指标。近年来,新型血液生物标志物被证明是进展的独立预测指标。本研究旨在评估这些新型标志物中哪一种在接受卡介苗免疫治疗的膀胱癌患者中具有最高的进展预后价值。
我们回顾性分析了125例接受卡介苗免疫治疗的非肌层浸润性膀胱癌患者的数据。其中,61例进展为肌层浸润性疾病或有高级别复发。将这些患者与未进展的组(n = 64)进行比较。收集了包括分期、分级、年龄、性别、吸烟状况和观察时间在内的临床数据。此外,从门诊数字病历中获取了血细胞计数分析信息。在此基础上,计算并比较了两组之间的中性粒细胞与淋巴细胞比值(NLR)、血小板与淋巴细胞比值(PLR)和淋巴细胞与单核细胞比值(LMR)。
在多变量分析中,NLR、PLR和LMR被证明是进展的独立预后标志物。包含分期、分级、年龄、性别、吸烟状况和LMR的模型在所有模型中具有最高的预后价值(曲线下面积[AUC] = 0.756)。根据LMR的ROC曲线,截断点为3.25。将LMR添加到包括临床变量的基线模型中,曲线下面积显著增加0.08(p = 0.001)。NLR和PLR未使曲线下面积相对于基线模型有显著增加。
在接受卡介苗免疫治疗的非肌层浸润性膀胱癌患者中,LMR在预测进展方面优于NLR和PLR。LMR作为一种易于获得的生物标志物,应纳入目前的风险分层模型中。