Department of Epidemiology and Biostatistics, Ministry of Education Key Laboratory of Environment and Health, State Key Laboratory of Environmental Health (Incubating), School of Public Health, Tongji Medical College, Huazhong University of Science and Technology, 430030 Wuhan, China.
Department of Epidemiology, School of Public Health, University of Michigan, Ann Arbor, MI, USA.
BMJ. 2021 Apr 14;373:n604. doi: 10.1136/bmj.n604.
To examine whether overall lifestyles mediate associations of socioeconomic status (SES) with mortality and incident cardiovascular disease (CVD) and the extent of interaction or joint relations of lifestyles and SES with health outcomes.
Population based cohort study.
US National Health and Nutrition Examination Survey (US NHANES, 1988-94 and 1999-2014) and UK Biobank.
44 462 US adults aged 20 years or older and 399 537 UK adults aged 37-73 years.
SES was derived by latent class analysis using family income, occupation or employment status, education level, and health insurance (US NHANES only), and three levels (low, medium, and high) were defined according to item response probabilities. A healthy lifestyle score was constructed using information on never smoking, no heavy alcohol consumption (women ≤1 drink/day; men ≤2 drinks/day; one drink contains 14 g of ethanol in the US and 8 g in the UK), top third of physical activity, and higher dietary quality.
All cause mortality was the primary outcome in both studies, and CVD mortality and morbidity in UK Biobank, which were obtained through linkage to registries.
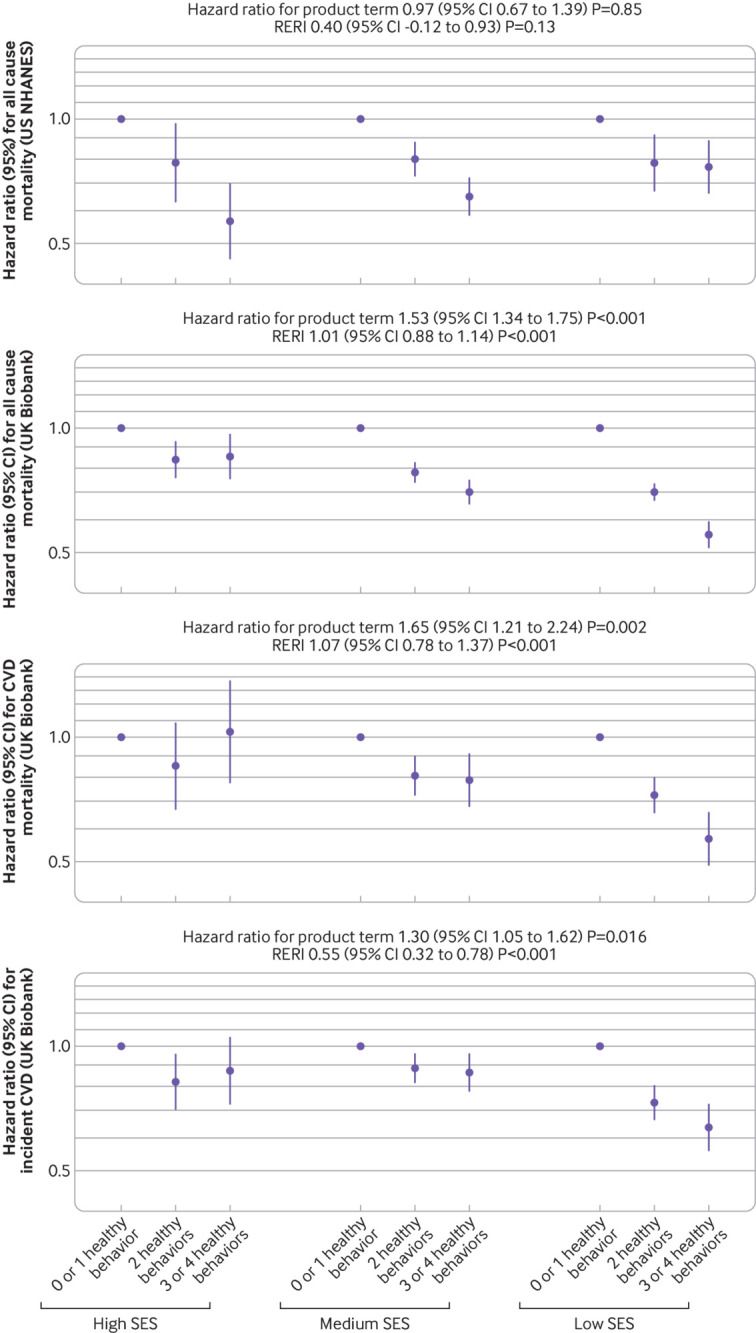
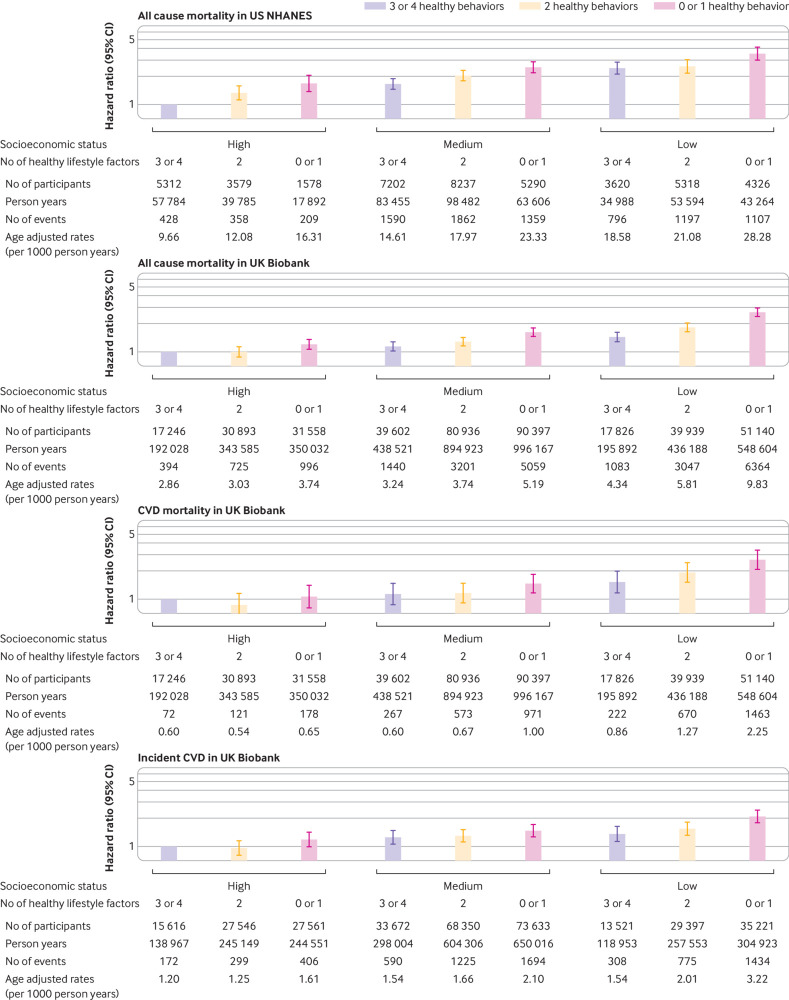
US NHANES documented 8906 deaths over a mean follow-up of 11.2 years, and UK Biobank documented 22 309 deaths and 6903 incident CVD cases over a mean follow-up of 8.8-11.0 years. Among adults of low SES, age adjusted risk of death was 22.5 (95% confidence interval 21.7 to 23.3) and 7.4 (7.3 to 7.6) per 1000 person years in US NHANES and UK Biobank, respectively, and age adjusted risk of CVD was 2.5 (2.4 to 2.6) per 1000 person years in UK Biobank. The corresponding risks among adults of high SES were 11.4 (10.6 to 12.1), 3.3 (3.1 to 3.5), and 1.4 (1.3 to 1.5) per 1000 person years. Compared with adults of high SES, those of low SES had higher risks of all cause mortality (hazard ratio 2.13, 95% confidence interval 1.90 to 2.38 in US NHANES; 1.96, 1.87 to 2.06 in UK Biobank), CVD mortality (2.25, 2.00 to 2.53), and incident CVD (1.65, 1.52 to 1.79) in UK Biobank, and the proportions mediated by lifestyle were 12.3% (10.7% to 13.9%), 4.0% (3.5% to 4.4%), 3.0% (2.5% to 3.6%), and 3.7% (3.1% to 4.5%), respectively. No significant interaction was observed between lifestyle and SES in US NHANES, whereas associations between lifestyle and outcomes were stronger among those of low SES in UK Biobank. Compared with adults of high SES and three or four healthy lifestyle factors, those with low SES and no or one healthy lifestyle factor had higher risks of all cause mortality (3.53, 3.01 to 4.14 in US NHANES; 2.65, 2.39 to 2.94 in UK Biobank), CVD mortality (2.65, 2.09 to 3.38), and incident CVD (2.09, 1.78 to 2.46) in UK Biobank.
Unhealthy lifestyles mediated a small proportion of the socioeconomic inequity in health in both US and UK adults; therefore, healthy lifestyle promotion alone might not substantially reduce the socioeconomic inequity in health, and other measures tackling social determinants of health are warranted. Nevertheless, healthy lifestyles were associated with lower mortality and CVD risk in different SES subgroups, supporting an important role of healthy lifestyles in reducing disease burden.
研究社会经济地位(SES)与死亡率和心血管疾病(CVD)发病率之间的关联是否受整体生活方式的影响,以及生活方式和 SES 与健康结果之间的相互作用或联合关系的程度。
基于人群的队列研究。
美国国家健康和营养调查(US NHANES,1988-94 年和 1999-2014 年)和英国生物银行。
44462 名年龄在 20 岁或以上的美国成年人和 399537 名年龄在 37-73 岁的英国成年人。
SES 通过使用家庭收入、职业或就业状况、教育水平和医疗保险(仅在美国 NHANES)的潜在类别分析得出,根据项目反应概率定义了低、中、高三个水平。使用从不吸烟、不大量饮酒(女性≤1 份/天;男性≤2 份/天;一份酒在美国含 14 克乙醇,在英国含 8 克乙醇)、活动量在前三分之一和更高的饮食质量构建健康生活方式评分。
两项研究的主要结局均为全因死亡率,英国生物银行的结局还包括 CVD 死亡率和发病率,通过与登记处的关联获得。
US NHANES 在平均 11.2 年的随访中记录了 8906 例死亡,英国生物银行在平均 8.8-11.0 年的随访中记录了 22309 例死亡和 6903 例 CVD 病例。在低 SES 的成年人中,美国 NHANES 和英国生物银行的年龄校正死亡风险分别为每 1000 人年 22.5(95%置信区间 21.7 至 23.3)和 7.4(7.3 至 7.6),英国生物银行的 CVD 风险为每 1000 人年 2.5(2.4 至 2.6)。高 SES 成年人的相应风险分别为 11.4(10.6 至 12.1)、3.3(3.1 至 3.5)和 1.4(1.3 至 1.5)。与高 SES 的成年人相比,低 SES 的成年人全因死亡率(风险比 2.13,95%置信区间 1.90 至 2.38)、CVD 死亡率(2.25,2.00 至 2.53)和 CVD 发病率(1.65,1.52 至 1.79)均较高,英国生物银行中生活方式介导的比例分别为 12.3%(10.7% 至 13.9%)、4.0%(3.5% 至 4.4%)、3.0%(2.5% 至 3.6%)和 3.7%(3.1% 至 4.5%)。在美国 NHANES 中,生活方式和 SES 之间没有明显的相互作用,而在英国生物银行中,生活方式与结局之间的关联在低 SES 人群中更强。与高 SES 的成年人和具有三个或四个健康生活方式因素的成年人相比,低 SES 且没有或只有一个健康生活方式因素的成年人全因死亡率(美国 NHANES 为 3.53,95%置信区间 3.01 至 4.14;英国生物银行为 2.65,95%置信区间 2.39 至 2.94)、CVD 死亡率(美国 NHANES 为 2.65,95%置信区间 2.09 至 3.38;英国生物银行为 2.65,95%置信区间 2.09 至 2.94)和 CVD 发病率(英国生物银行为 2.09,95%置信区间 1.78 至 2.46)的风险更高。
不健康的生活方式在一定程度上解释了美国和英国成年人健康方面的社会经济不平等;因此,仅促进健康的生活方式可能不会显著降低社会经济不平等对健康的影响,需要采取其他措施来解决健康决定因素的社会决定因素。然而,在不同 SES 亚组中,健康的生活方式与较低的死亡率和 CVD 风险相关,支持健康生活方式在降低疾病负担方面的重要作用。