Huang Ying-Jhen, Chu Yi-Chi, Huang Hung-Ling, Hwang Jing-Shiang, Chan Ta-Chien
Research Center for Humanities and Social Sciences, Academia Sinica, Taipei, Taiwan.
Kaohsiung Municipal Ta-Tung Hospital, Kaohsiung, Taiwan.
J Asthma Allergy. 2021 Apr 8;14:347-359. doi: 10.2147/JAA.S299186. eCollection 2021.
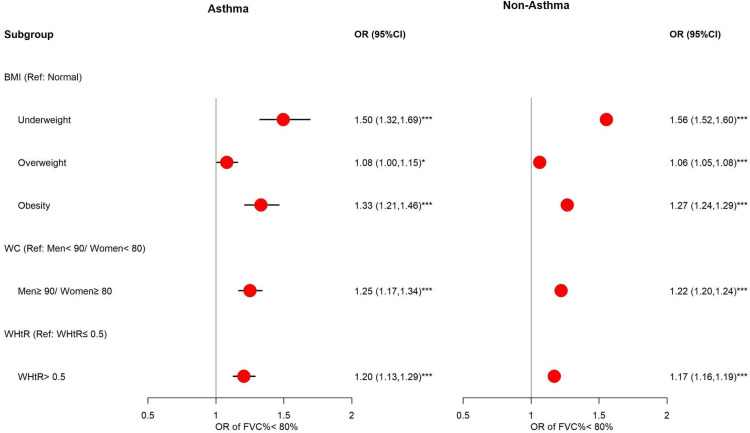
Asthma and obesity are important public health issues around the world. Obesity is considered a risk factor associated with the severity and incidence of asthma. We investigated the relationships between poor pulmonary function (defined by forced vital capacity (FVC) and percentage of predicted FVC (FVC%)) and obesity.
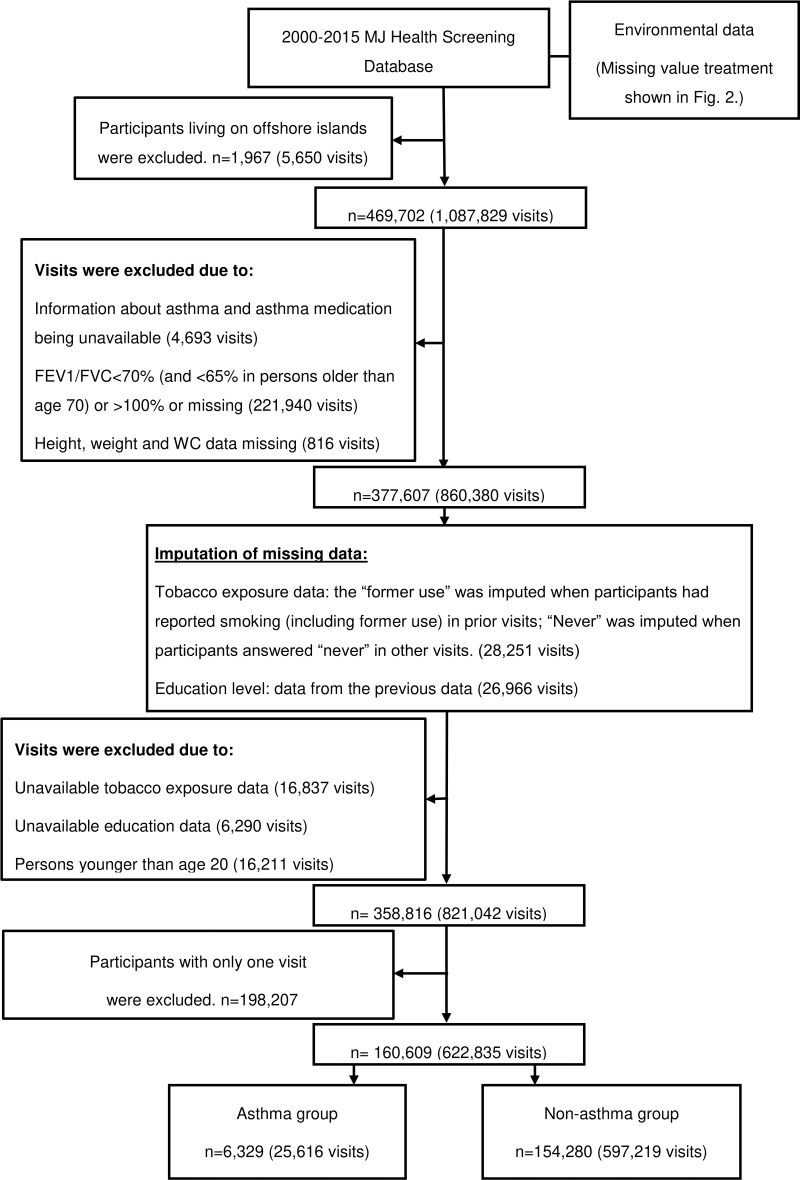
This is a retrospective longitudinal study using the MJ health examination database in Taiwan from 2000 to 2015. There were 160,609 participants aged ≥20 years with complete obesity indicators and lung function data, and having at least two visits. A generalized estimation equation (GEE) model was applied to estimate the association between lung function and obesity.
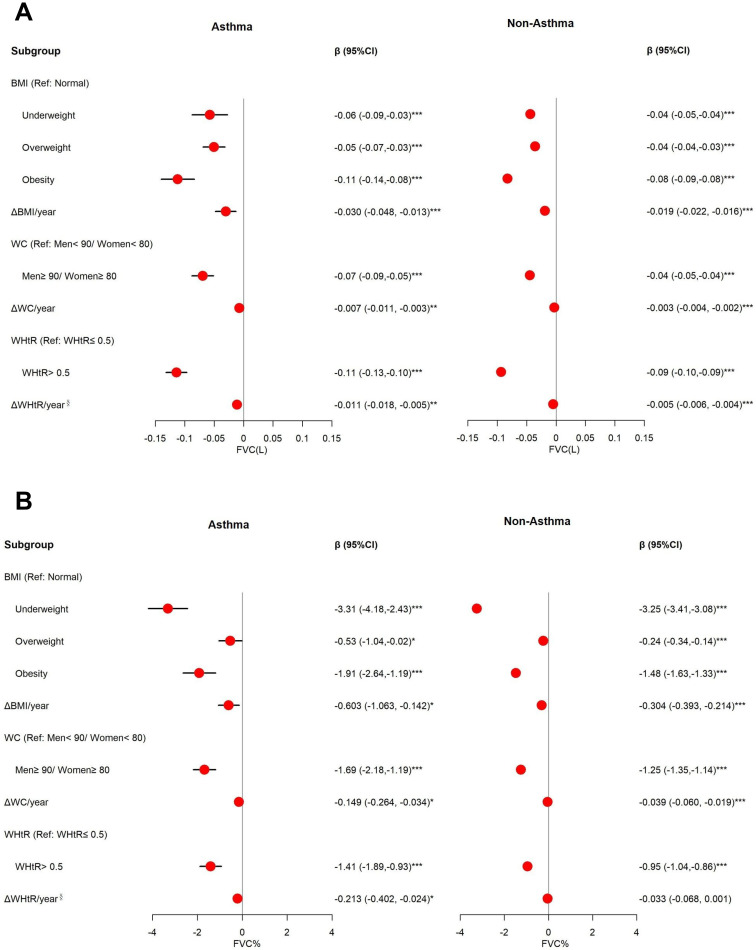
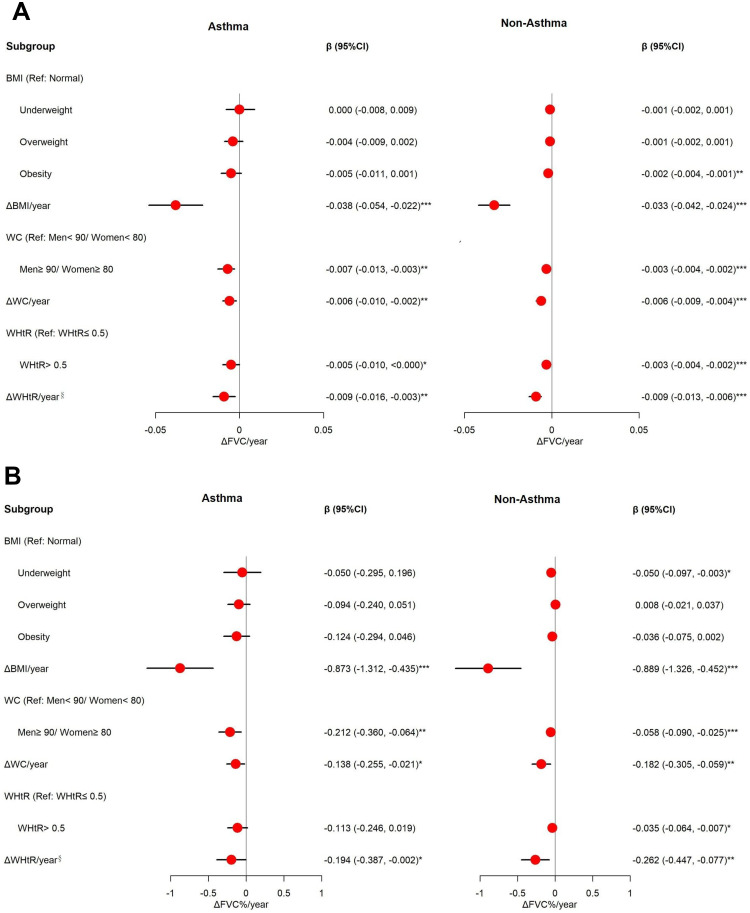
BMI was the best indicator to predict poor pulmonary function for our participants. Results of BMI are presented as an example: Obesity (body mass index (BMI) ≥27.0 kg/m) is significantly associated with lower FVC [adjusted coefficients (β) for asthmatics: -0.11 L (95% CI: -0.14, -0.08); adjusted β for non-asthmatics: -0.08 L (-0.09, -0.08)] and FVC% [adjusted β for asthmatics: -1.91% (95% CI: -2.64, -1.19); adjusted β for non-asthmatics: 1.48% (-1.63, -1.33)]. Annual change of BMI (ΔBMI/year) is an independent risk factor for decreased FVC [adjusted β for asthmatics: -0.030 L (-0.048, -0.013); adjusted β for non-asthmatics: -0.019 L (-0.022, -0.016)] and FVC% [adjusted β for non-asthmatics: -0.603% (-1.063, -0.142); adjusted β for non-asthmatics: -0.304% (-0.393, -0.214)], and is significantly associated with accelerated FVC decline [adjusted β of ΔFVC/year and ΔFVC %/year for asthmatics: -0.038 L (-0.054, -0.022) and -0.873% (-1.312, -0.435); adjusted β of ΔFVC/year and ΔFVC %/year for non-asthmatics: -0.033 L (-0.042, -0.024) and -0.889% (-1.326, -0.452)].
Obesity is significantly associated with decreased lung function, and asthmatics had a higher risk than non-asthmatics.
哮喘和肥胖是全球重要的公共卫生问题。肥胖被认为是与哮喘严重程度和发病率相关的风险因素。我们研究了肺功能差(由用力肺活量(FVC)和预测FVC百分比(FVC%)定义)与肥胖之间的关系。
这是一项回顾性纵向研究,使用了台湾2000年至2015年的MJ健康检查数据库。共有160,609名年龄≥20岁的参与者,他们具有完整的肥胖指标和肺功能数据,且至少有两次就诊记录。应用广义估计方程(GEE)模型来估计肺功能与肥胖之间的关联。
BMI是预测我们研究参与者肺功能差的最佳指标。以BMI的结果为例:肥胖(体重指数(BMI)≥27.0 kg/m²)与较低的FVC显著相关[哮喘患者的调整系数(β):-0.11 L(95%置信区间:-0.14,-0.08);非哮喘患者的调整β:-0.08 L(-0.09,-0.08)]和FVC%[哮喘患者的调整β:-1.91%(95%置信区间:-2.64,-1.19);非哮喘患者的调整β:-1.48%(-1.63,-1.33)]。BMI的年度变化(ΔBMI/年)是FVC降低的独立风险因素[哮喘患者的调整β:-0.030 L(-0.048,-0.013);非哮喘患者的调整β:-0.019 L(-0.022,-0.016)]和FVC%[非哮喘患者的调整β:-0.603%(-1.063,-0.142);非哮喘患者的调整β:-0.304%(-0.393,-0.214)],并且与FVC加速下降显著相关[哮喘患者的ΔFVC/年和ΔFVC %/年的调整β:-0.038 L(-0.054,-0.022)和-0.873%(-1.312,-0.435);非哮喘患者的ΔFVC/年和ΔFVC %/年的调整β:-0.033 L(-0.042,-0.024)和-0.889%(-1.326,-0.452)]。
肥胖与肺功能下降显著相关,哮喘患者比非哮喘患者风险更高。