Shouman Kamal, Vanichkachorn Greg, Cheshire William P, Suarez Mariana D, Shelly Shahar, Lamotte Guillaume J, Sandroni Paola, Benarroch Eduardo E, Berini Sarah E, Cutsforth-Gregory Jeremy K, Coon Elizabeth A, Mauermann Michelle L, Low Phillip A, Singer Wolfgang
Department of Neurology, Mayo Clinic, 200 First Street SW, Rochester, MN, 55905, USA.
Preventive, Occupational, and Aerospace Medicine, Mayo Clinic, 200 First Street SW, Rochester, MN, 55905, USA.
Clin Auton Res. 2021 Jun;31(3):385-394. doi: 10.1007/s10286-021-00803-8. Epub 2021 Apr 16.
Post-COVID-19 syndrome is a poorly understood aspect of the current pandemic, with clinical features that overlap with symptoms of autonomic/small fiber dysfunction. An early systematic analysis of autonomic dysfunction following COVID-19 is lacking and may provide initial insights into the spectrum of this condition.
We conducted a retrospective review of all patients with confirmed history of COVID-19 infection referred for autonomic testing for symptoms concerning for para-/postinfectious autonomic dysfunction at Mayo Clinic Rochester or Jacksonville between March 2020 and January 2021.
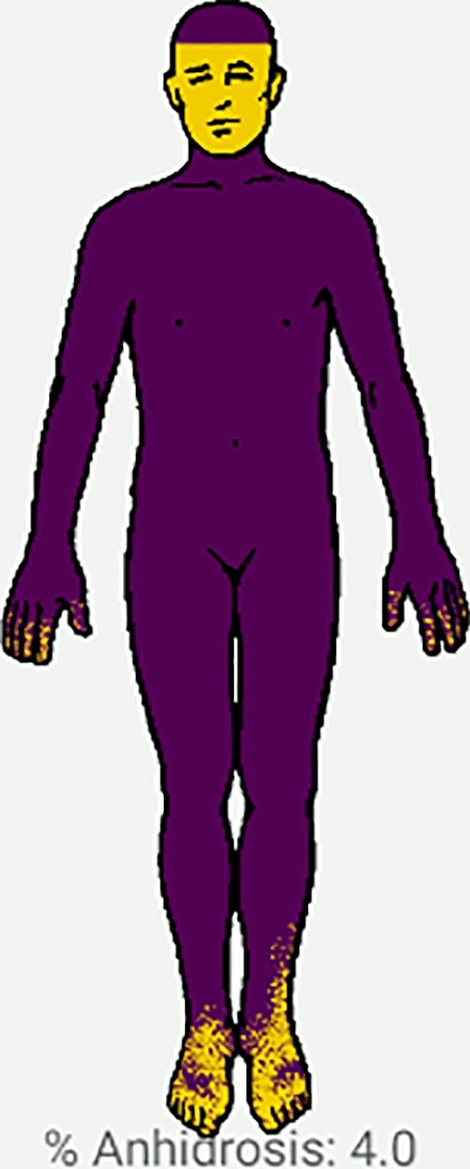
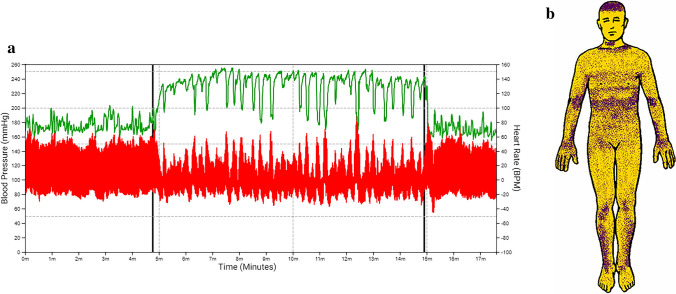
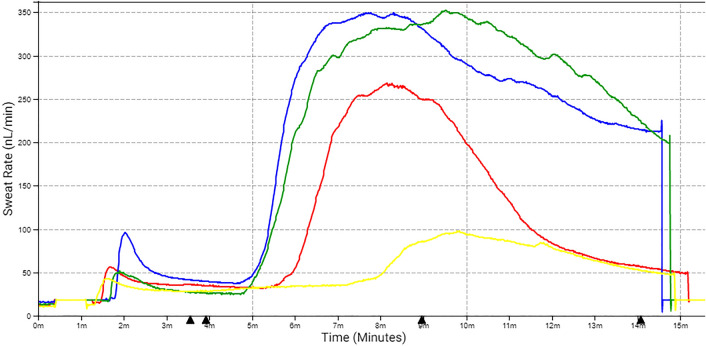
We identified 27 patients fulfilling the search criteria. Symptoms developed between 0 and 122 days following the acute infection and included lightheadedness (93%), orthostatic headache (22%), syncope (11%), hyperhidrosis (11%), and burning pain (11%). Sudomotor function was abnormal in 36%, cardiovagal function in 27%, and cardiovascular adrenergic function in 7%. The most common clinical scenario was orthostatic symptoms without tachycardia or hypotension (41%); 22% of patients fulfilled the criteria for postural tachycardia syndrome (POTS), and 11% had borderline findings to support orthostatic intolerance. One patient each was diagnosed with autoimmune autonomic ganglionopathy, inappropriate sinus tachycardia, vasodepressor syncope, cough/vasovagal syncope, exacerbation of preexisting orthostatic hypotension, exacerbation of sensory and autonomic neuropathy, and exacerbation of small fiber neuropathy.
Abnormalities on autonomic testing were seen in the majority of patients but were mild in most cases. The most common finding was orthostatic intolerance, often without objective hemodynamic abnormalities on testing. Unmasking/exacerbation of preexisting conditions was seen. The temporal association between infection and autonomic symptoms implies a causal relationship, which however cannot be proven by this study.
新冠后综合征是当前大流行中一个尚未被充分理解的方面,其临床特征与自主神经/小纤维功能障碍的症状重叠。目前缺乏对新冠后自主神经功能障碍的早期系统分析,而这可能为该病症的范围提供初步见解。
我们对2020年3月至2021年1月期间在梅奥诊所罗切斯特或杰克逊维尔因疑似感染后自主神经功能障碍症状而接受自主神经测试的所有确诊新冠感染病史患者进行了回顾性研究。
我们确定了27名符合搜索标准的患者。症状在急性感染后的0至122天出现,包括头晕(93%)、直立性头痛(22%)、晕厥(11%)、多汗(11%)和灼痛(11%)。汗腺运动功能异常的占36%,心脏迷走神经功能异常的占27%,心血管肾上腺素能功能异常的占7%。最常见的临床情况是直立性症状但无心动过速或低血压(41%);22%的患者符合姿势性心动过速综合征(POTS)标准,11%的患者有临界结果支持直立不耐受。各有1例患者被诊断为自身免疫性自主神经节病、不适当窦性心动过速、血管减压性晕厥、咳嗽/血管迷走性晕厥、既往直立性低血压加重、感觉和自主神经病变加重以及小纤维神经病变加重。
大多数患者的自主神经测试存在异常,但大多数情况下症状较轻。最常见的发现是直立不耐受,测试时通常无客观血流动力学异常。发现了既往病症的暴露/加重情况。感染与自主神经症状之间的时间关联意味着因果关系,但本研究无法证实这一点。