Falster Casper, Jacobsen Niels, Wulff Madsen Lone, Dahlerup Rasmussen Line, Davidsen Jesper Rømhild, Christie Knudtzen Fredrikke, Nielsen Stig Lønberg, Johansen Isik Somuncu, Laursen Christian B
Department of Respiratory Medicine, Odense University Hospital, Odense, Denmark.
Odense Respiratory Research Unit (ODIN), Department of Clinical Research, Health Sciences, University of Southern Denmark, Odense, Denmark.
Eur Clin Respir J. 2021 Apr 7;8(1):1909521. doi: 10.1080/20018525.2021.1909521.
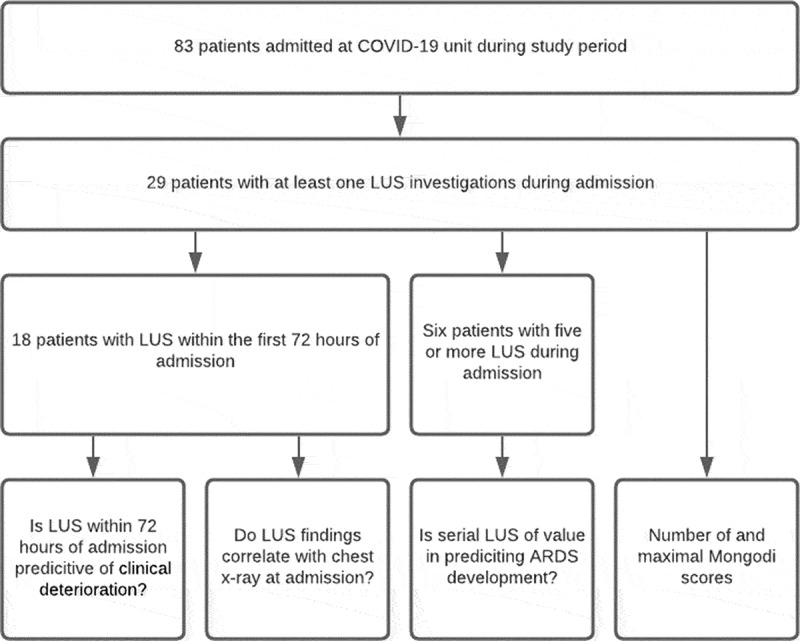
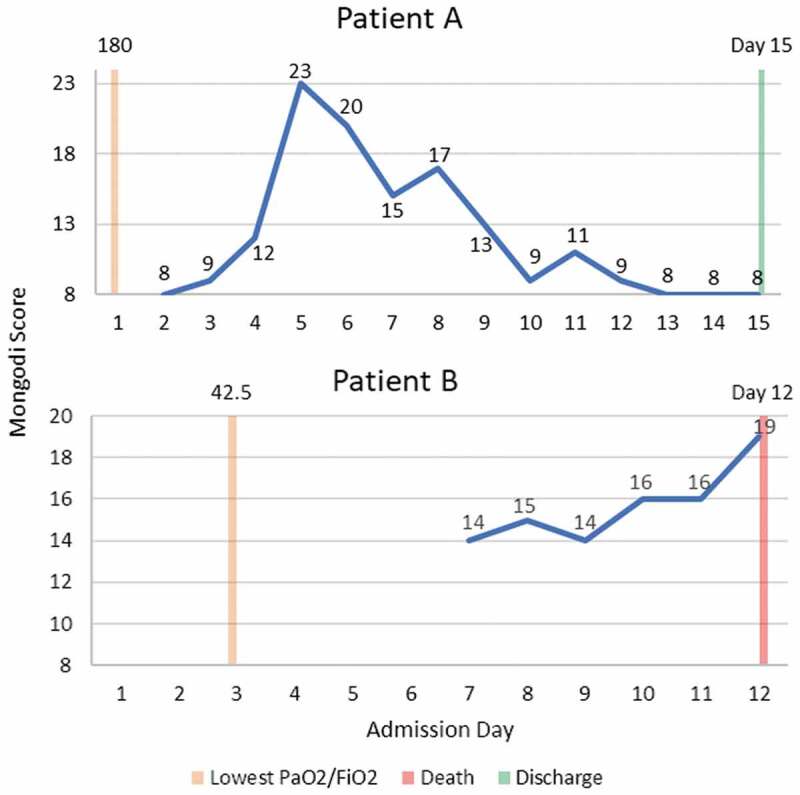
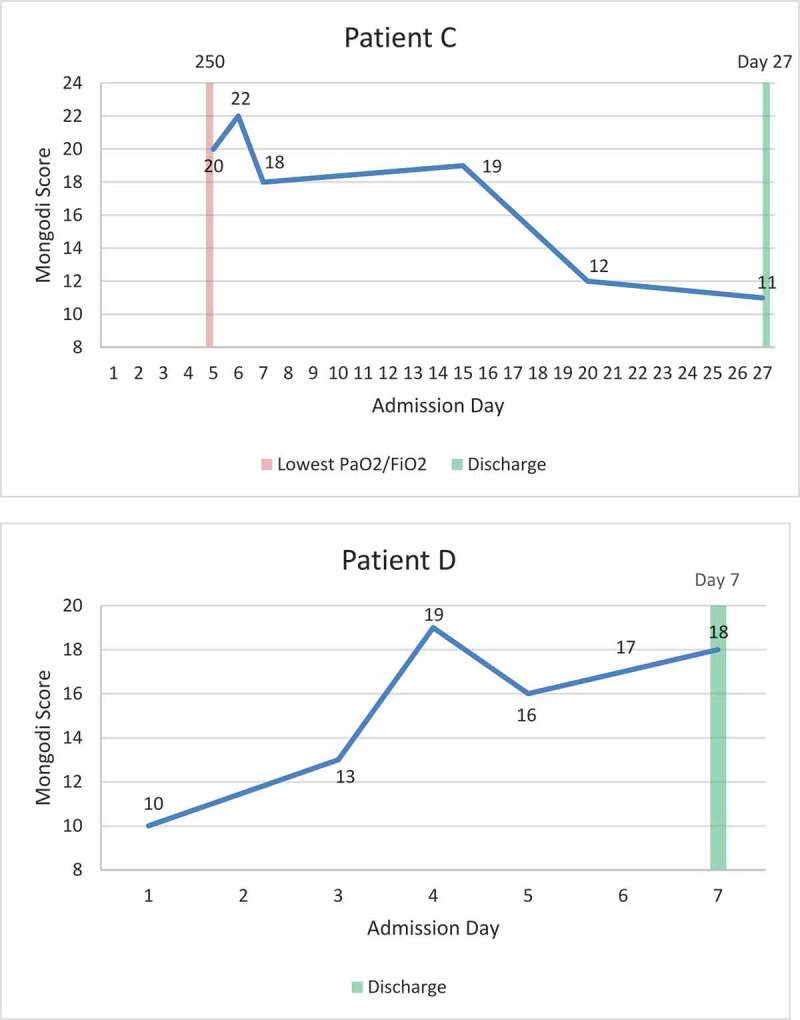
COVID-19 is associated with a risk of severe pneumonia and acute respiratory distress syndrome (ARDS), requiring treatment at an intensive care unit (ICU). Since clinical deterioration may occur rapidly, a simple, fast, bedside, non-invasive method for assessment of lung changes is warranted. The primary aim of this study was to investigate whether lung ultrasound (LUS) findings within 72 hours of admission were predictive of clinical deterioration in hospitalized patients with confirmed Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). Patients admitted to a dedicated COVID-19 unit were subject to daily LUS examinations. Number of present consolidations and pleural effusions were registered and a Mongodi score was calculated. These findings were correlated with initial chest x-ray and clinical deterioration, defined as ICU-admission, ARDS diagnosis, death. In total, 29 of 83 patients had LUS performed during admission, 18 within 72 h of admission. Of these, four patients died during admission, six were transferred to the ICU and 13 were diagnosed with ARDS. Initial Mongodi-score did not differ significantly between patients with and without clinical deterioration (p = 0.95). Agreement between initial LUS and chest x-ray findings were fair with Cohen's Kappa at 0.21. LUS performed within 72 h in patients admitted to a dedicated COVID-19 unit could not predict ARDS, ICU admission or death. However, consecutive investigations may be of value, as sudden substantial changes may herald disease progression, enabling earlier supplementary diagnostics and treatment initiation.
新型冠状病毒肺炎(COVID-19)与严重肺炎及急性呼吸窘迫综合征(ARDS)风险相关,需要在重症监护病房(ICU)进行治疗。由于临床病情可能迅速恶化,因此需要一种简单、快速、床旁、非侵入性的肺部变化评估方法。本研究的主要目的是调查确诊感染严重急性呼吸综合征冠状病毒2(SARS-CoV-2)的住院患者入院72小时内的肺部超声(LUS)检查结果是否可预测临床病情恶化。入住专门的COVID-19病房的患者每天接受LUS检查。记录实变和胸腔积液的数量,并计算蒙戈迪评分。这些检查结果与初始胸部X线检查结果及临床病情恶化情况相关,临床病情恶化定义为入住ICU、诊断为ARDS或死亡。总共83例患者中有29例在住院期间接受了LUS检查,其中18例在入院72小时内接受检查。在这些患者中,4例在住院期间死亡,6例转入ICU,13例被诊断为ARDS。有临床病情恶化和无临床病情恶化的患者初始蒙戈迪评分无显著差异(p = 0.95)。初始LUS检查结果与胸部X线检查结果之间的一致性一般,科恩kappa系数为0.21。入住专门的COVID-19病房的患者在72小时内进行的LUS检查无法预测ARDS、入住ICU或死亡。然而,连续检查可能有价值,因为突然的显著变化可能预示疾病进展,从而能够更早地进行补充诊断和开始治疗。