Monlezun Dominique J, Lawless Sean, Palaskas Nicolas, Peerbhai Shareez, Charitakis Konstantinos, Marmagkiolis Konstantinos, Lopez-Mattei Juan, Mamas Mamas, Iliescu Cezar
Department of Cardiology, The University of Texas M.D. Anderson Cancer Center, Houston, TX, United States.
Division of Cardiovascular Medicine, The University of Texas Health Sciences Center at Houston, Houston, TX, United States.
Front Cardiovasc Med. 2021 Apr 6;8:620857. doi: 10.3389/fcvm.2021.620857. eCollection 2021.
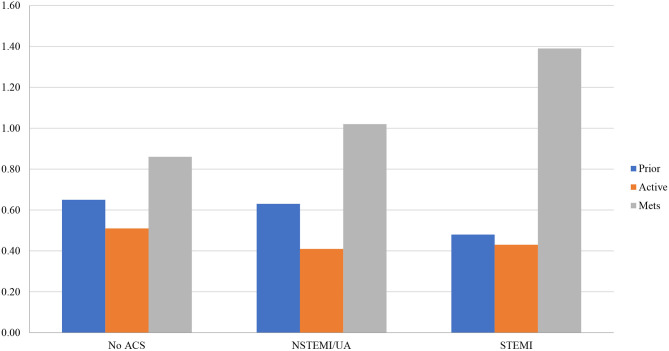
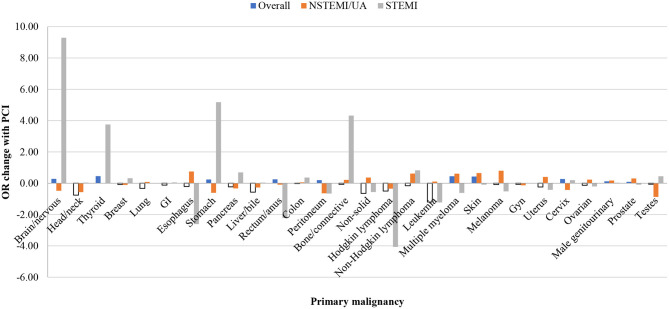
It is unknown to what extent the clinical benefits of PCI outweigh the risks and costs in patients with vs. without cancer and within each cancer type. We performed the first known nationally representative propensity score analysis of PCI mortality and cost among all eligible adult inpatients by cancer and its types. This multicenter case-control study used machine learning-augmented propensity score-adjusted multivariable regression to assess the above outcomes and disparities using the 2016 nationally representative National Inpatient Sample. Of the 30,195,722 hospitalized patients, 15.43% had a malignancy, 3.84% underwent an inpatient PCI (of whom 11.07% had cancer and 0.07% had metastases), and 2.19% died inpatient. In fully adjusted analyses, PCI vs. medical management significantly reduced mortality for patients overall (among all adult inpatients regardless of cancer status) and specifically for cancer patients (OR 0.82, 95% CI 0.75-0.89; < 0.001), mainly driven by active vs. prior malignancy, head and neck and hematological malignancies. PCI also significantly reduced cancer patients' total hospitalization costs (beta USD$ -8,668.94, 95% CI -9,553.59 to -7,784.28; < 0.001) independent of length of stay. There were no significant income or disparities among PCI subjects. Our study suggests among all eligible adult inpatients, PCI does not increase mortality or cost for cancer patients, while there may be particular benefit by cancer type. The presence or history of cancer should not preclude these patients from indicated cardiovascular care.
在患有和未患癌症的患者以及每种癌症类型中,经皮冠状动脉介入治疗(PCI)的临床益处超过风险和成本的程度尚不清楚。我们对所有符合条件的成年住院患者按癌症及其类型进行了首次全国代表性的PCI死亡率和成本倾向评分分析。这项多中心病例对照研究使用机器学习增强的倾向评分调整多变量回归,通过2016年全国代表性的国家住院样本评估上述结果和差异。在30195722名住院患者中,15.43%患有恶性肿瘤,3.84%接受了住院PCI(其中11.07%患有癌症,0.07%有转移),2.19%住院死亡。在完全调整分析中,PCI与药物治疗相比,显著降低了总体患者(所有成年住院患者,无论癌症状态如何)尤其是癌症患者的死亡率(比值比0.82,95%置信区间0.75 - 0.89;P < 0.001),主要由现患与既往恶性肿瘤、头颈部和血液系统恶性肿瘤驱动。PCI还显著降低了癌症患者的总住院费用(β - 8668.94美元,95%置信区间 - 9553.59至 - 7784.28;P < 0.001),且与住院时间无关。PCI受试者之间没有显著的收入差异。我们的研究表明,在所有符合条件的成年住院患者中,PCI不会增加癌症患者的死亡率或成本,而可能因癌症类型有特定益处。癌症的存在或病史不应妨碍这些患者接受必要的心血管治疗。