Department of Hepatology, Toranomon Hospital, Okinaka Memorial Institute for Medical Research, 2-2-2 Toranomon, Minato-ku, Tokyo, 105-0001, Japan.
Liver Research Laboratory, Toranomon Hospital, Tokyo, Japan.
BMC Gastroenterol. 2021 Apr 23;21(1):189. doi: 10.1186/s12876-021-01770-0.
Hepatitis C virus is the leading cause of liver cirrhosis and hepatocellular carcinoma in Japan. We aimed to examine the long-term (> 20 years) mortality and hepatocellular carcinoma rates and associated risk factors in 1412 Japanese patients with decompensated hepatitis C virus-related cirrhosis (Child-Pugh B or C).
Cumulative survival and hepatocellular carcinoma rates were determined using Kaplan-Meier analysis. Independent risk factors were identified by multivariate analysis. A two-tailed P-value of < 0.05 was considered significant.
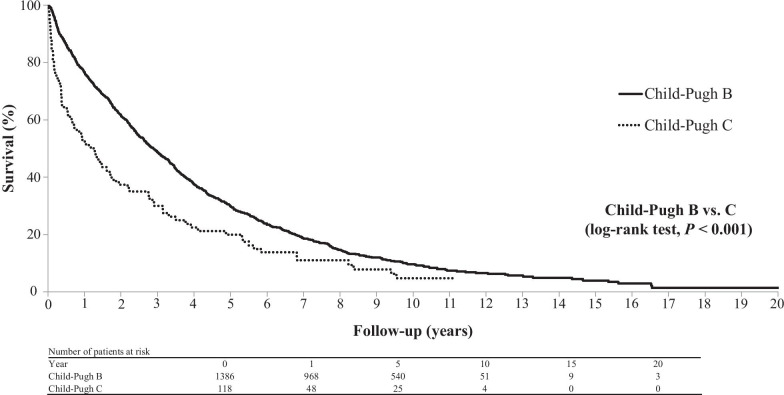
The patients were followed up for a median of 2 years (range 0.5-24.2 years). In total, 62.3%, 41.7%, 4.7%, and 68.3% of the patients had a history of hepatocellular carcinoma, ascites, hepatic encephalopathy, and esophageal varices, respectively. The 1-, 5-, 10-, and 20-year cumulative overall survival rates in the total cohort was 74.9%, 29.0%, 9.1%, and 1.4%, respectively. The 1-, 3-, 5-, and 10-year cumulative survival rates for patients without hepatocellular carcinoma were 93.1%, 54.4%, 18.2%, and 4.0%, respectively, and the corresponding cumulative post-decompensation hepatocellular carcinoma rates were 14.0%, 31.6%, 46.1%, and 66.2%, respectively. The independent risk factors for mortality were older age, Child-Pugh C cirrhosis, the presence of hepatocellular carcinoma, low estimated glomerular filtration rate, low serum sodium level, low platelet count, and high γ-glutamyl transferase and α-fetoprotein levels for all patients and older age, Child-Pugh C cirrhosis, and low estimated glomerular filtration rate for patients without hepatocellular carcinoma. Overall, 1035 patients (73.3%) died; the causes of death were liver failure with/without hepatocellular carcinoma, pneumonia, sepsis, cardiovascular disease, and non-hepatocellular carcinoma malignancies. The corresponding morality rates per person-year were 133.4, 59.9, 10.9, 10.6, 9.0, and 5.2, respectively.
Among Japanese patients with decompensated hepatitis C virus-related cirrhosis, hepatocellular carcinoma is associated with poor prognosis. Our results highlight the importance of managing liver-related events, including hepatocellular carcinoma, in these patients.
丙型肝炎病毒是日本肝硬化和肝细胞癌的主要病因。我们旨在研究 1412 例失代偿性丙型肝炎病毒相关肝硬化(Child-Pugh B 或 C)患者的长期(>20 年)死亡率和肝细胞癌发生率及其相关危险因素。
采用 Kaplan-Meier 分析确定累积生存率和肝细胞癌发生率。通过多因素分析确定独立的危险因素。双侧 P 值<0.05 认为具有统计学意义。
患者中位随访时间为 2 年(0.5-24.2 年)。总共有 62.3%、41.7%、4.7%和 68.3%的患者分别有肝细胞癌、腹水、肝性脑病和食管静脉曲张病史。全队列 1、5、10 和 20 年的累积总生存率分别为 74.9%、29.0%、9.1%和 1.4%。无肝细胞癌患者的 1、3、5 和 10 年累积生存率分别为 93.1%、54.4%、18.2%和 4.0%,相应的失代偿后肝细胞癌累积发生率分别为 14.0%、31.6%、46.1%和 66.2%。所有患者死亡的独立危险因素为年龄较大、Child-Pugh C 肝硬化、存在肝细胞癌、估算肾小球滤过率低、血清钠水平低、血小板计数低、γ-谷氨酰转移酶和甲胎蛋白水平高,而无肝细胞癌患者的独立危险因素为年龄较大、Child-Pugh C 肝硬化和估算肾小球滤过率低。总体而言,1035 例患者(73.3%)死亡;死亡原因包括伴/不伴肝细胞癌的肝功能衰竭、肺炎、败血症、心血管疾病和非肝细胞癌恶性肿瘤。相应的每患者人年死亡率分别为 133.4、59.9、10.9、10.6、9.0 和 5.2。
在日本失代偿性丙型肝炎病毒相关肝硬化患者中,肝细胞癌与预后不良相关。我们的研究结果强调了管理这些患者肝脏相关事件(包括肝细胞癌)的重要性。