Jayasimhan Dilip, Foster Simon, Chang Catherina L, Hancox Robert J
Respiratory Research Unit, Department of Respiratory Medicine, Waikato Hospital, Pembroke Street, Hamilton, 3204, New Zealand.
Department of Preventative and Social Medicine, Otago Medical School, University of Otago, Dunedin, New Zealand.
J Intensive Care. 2021 Apr 26;9(1):36. doi: 10.1186/s40560-021-00548-6.
Acute respiratory distress syndrome (ARDS) is a leading cause of morbidity and mortality in the intensive care unit. Biochemical markers of cardiac dysfunction are associated with high mortality in many respiratory conditions. The aim of this systematic review is to examine the link between elevated biomarkers of cardiac dysfunction in ARDS and mortality.
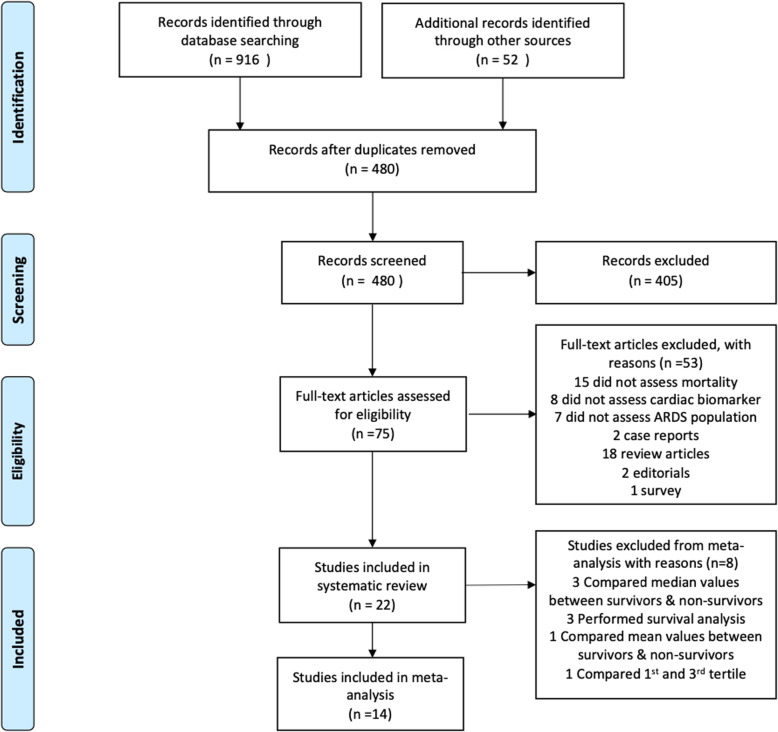
A systematic review of MEDLINE, EMBASE, Web of Science and CENTRAL databases was performed. We included studies of adult intensive care patients with ARDS that reported the risk of death in relation to a measured biomarker of cardiac dysfunction. The primary outcome of interest was mortality up to 60 days. A random-effects model was used for pooled estimates. Funnel-plot inspection was done to evaluate publication bias; Cochrane chi-square tests and I tests were used to assess heterogeneity.
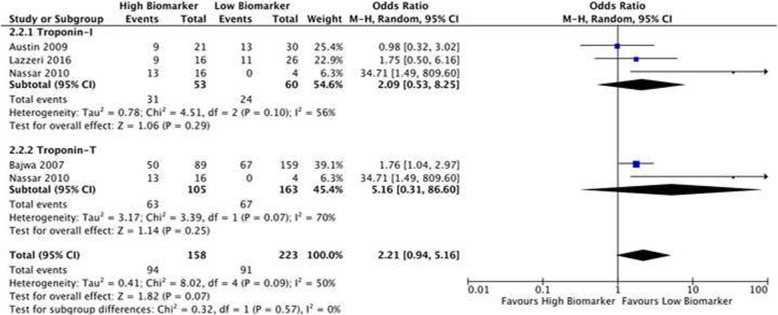
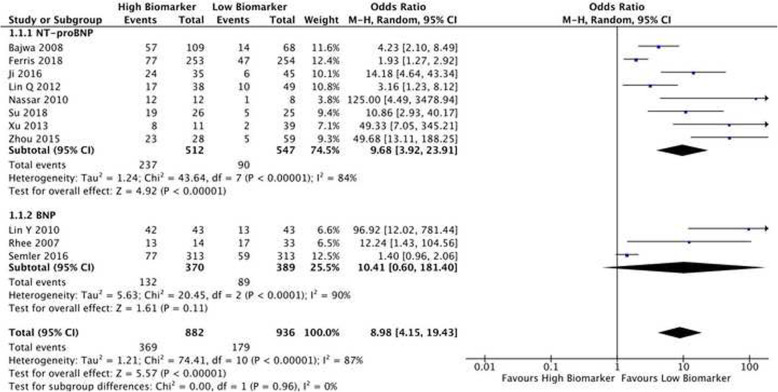
Twenty-two studies were included in the systematic review and 18 in the meta-analysis. Biomarkers of cardiac stretch included NT-ProBNP (nine studies) and BNP (six studies). Biomarkers of cardiac injury included Troponin-T (two studies), Troponin-I (one study) and High-Sensitivity-Troponin-I (three studies). Three studies assessed multiple cardiac biomarkers. High levels of NT-proBNP and BNP were associated with a higher risk of death up to 60 days (unadjusted OR 8.98; CI 4.15-19.43; p<0.00001). This association persisted after adjustment for age and illness severity. Biomarkers of cardiac injury were also associated with higher mortality, but this association was not statistically significant (unadjusted OR 2.21; CI 0.94-5.16; p= 0.07).
Biomarkers of cardiac stretch are associated with increased mortality in ARDS.
急性呼吸窘迫综合征(ARDS)是重症监护病房发病和死亡的主要原因。心脏功能障碍的生化标志物与许多呼吸系统疾病的高死亡率相关。本系统评价的目的是研究ARDS中心脏功能障碍生物标志物升高与死亡率之间的联系。
对MEDLINE、EMBASE、科学网和CENTRAL数据库进行系统评价。我们纳入了关于成人ARDS重症监护患者的研究,这些研究报告了与所测量的心脏功能障碍生物标志物相关的死亡风险。感兴趣的主要结局是60天内的死亡率。采用随机效应模型进行合并估计。通过漏斗图检查评估发表偏倚;采用Cochrane卡方检验和I²检验评估异质性。
系统评价纳入22项研究,荟萃分析纳入18项研究。心脏扩张生物标志物包括N末端B型利钠肽原(NT-ProBNP,9项研究)和B型利钠肽(BNP,6项研究)。心脏损伤生物标志物包括肌钙蛋白T(2项研究)、肌钙蛋白I(1项研究)和高敏肌钙蛋白I(3项研究)。3项研究评估了多种心脏生物标志物。NT-proBNP和BNP水平升高与60天内较高的死亡风险相关(未调整的比值比8.98;可信区间4.15 - 19.43;p<0.00001)。在调整年龄和疾病严重程度后,这种关联仍然存在。心脏损伤生物标志物也与较高的死亡率相关,但这种关联无统计学意义(未调整的比值比:2.21;可信区间0.94 - 5.16;p = 0.07)。
心脏扩张生物标志物与ARDS患者死亡率增加相关。