Academic Unit of Primary Care, Population Sciences and Medical Education, Faculty of Medicine, University of Southampton, Southampton, UK.
Biostatistics Research Group, Department of Health Sciences, College of Life Sciences, University of Leicester, Leicester, UK.
BMJ. 2021 Apr 28;373:n808. doi: 10.1136/bmj.n808.
To assess the overall effect of delayed antibiotic prescribing on average symptom severity for patients with respiratory tract infections in the community, and to identify any factors modifying this effect.
Systematic review and individual patient data meta-analysis.
Cochrane Central Register of Controlled Trials, Ovid Medline, Ovid Embase, EBSCO CINAHL Plus, and Web of Science.
Randomised controlled trials and observational cohort studies in a community setting that allowed comparison between delayed versus no antibiotic prescribing, and delayed versus immediate antibiotic prescribing.
The primary outcome was the average symptom severity two to four days after the initial consultation measured on a seven item scale (ranging from normal to as bad as could be). Secondary outcomes were duration of illness after the initial consultation, complications resulting in admission to hospital or death, reconsultation with the same or worsening illness, and patient satisfaction rated on a Likert scale.
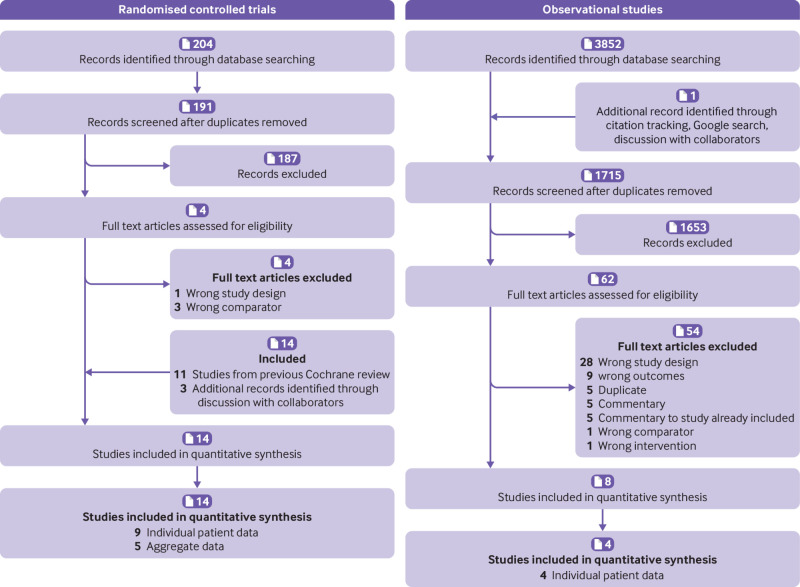
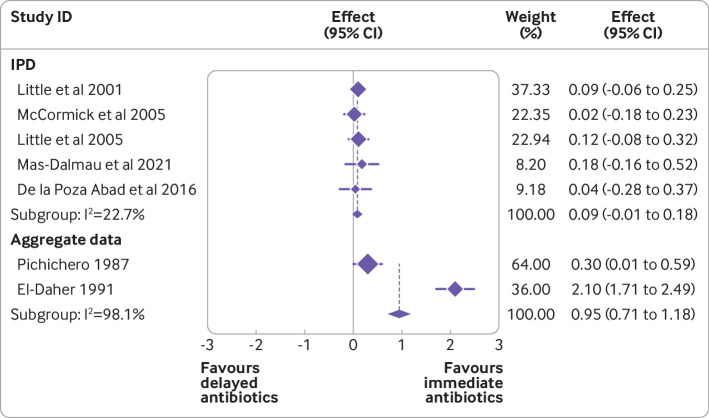
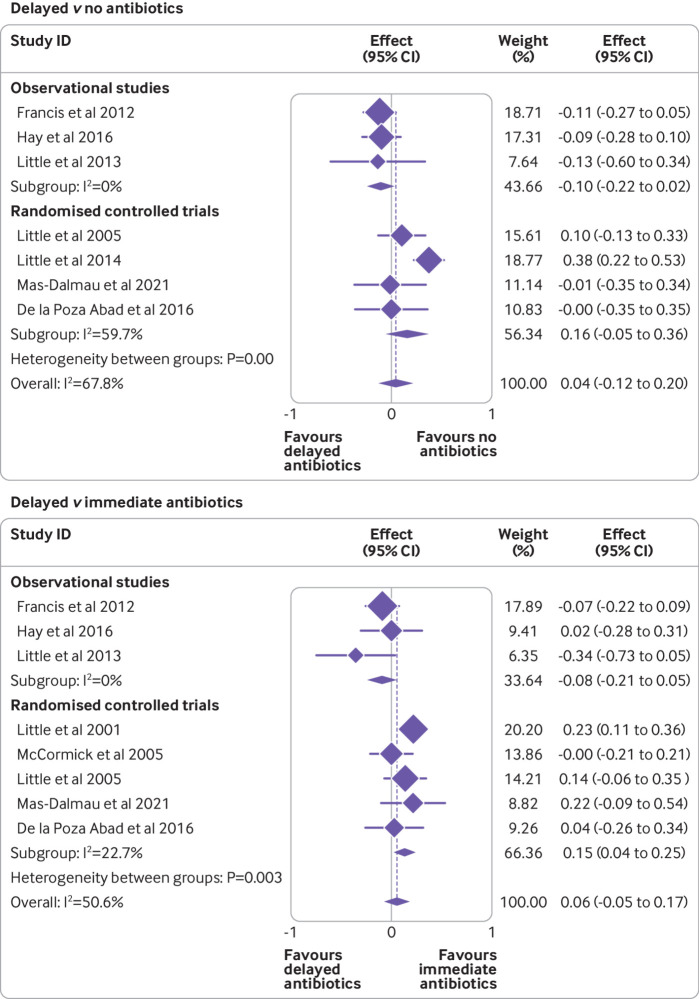
Data were obtained from nine randomised controlled trials and four observational studies, totalling 55 682 patients. No difference was found in follow-up symptom severity (seven point scale) for delayed versus immediate antibiotics (adjusted mean difference -0.003, 95% confidence interval -0.12 to 0.11) or delayed versus no antibiotics (0.02, -0.11 to 0.15). Symptom duration was slightly longer in those given delayed versus immediate antibiotics (11.4 10.9 days), but was similar for delayed versus no antibiotics. Complications resulting in hospital admission or death were lower with delayed versus no antibiotics (odds ratio 0.62, 95% confidence interval 0.30 to 1.27) and delayed versus immediate antibiotics (0.78, 0.53 to 1.13). A significant reduction in reconsultation rates (odds ratio 0.72, 95% confidence interval 0.60 to 0.87) and an increase in patient satisfaction (adjusted mean difference 0.09, 0.06 to 0.11) were observed in delayed versus no antibiotics. The effect of delayed versus immediate antibiotics and delayed versus no antibiotics was not modified by previous duration of illness, fever, comorbidity, or severity of symptoms. Children younger than 5 years had a slightly higher follow-up symptom severity with delayed antibiotics than with immediate antibiotics (adjusted mean difference 0.10, 95% confidence interval 0.03 to 0.18), but no increased severity was found in the older age group.
Delayed antibiotic prescribing is a safe and effective strategy for most patients, including those in higher risk subgroups. Delayed prescribing was associated with similar symptom duration as no antibiotic prescribing and is unlikely to lead to poorer symptom control than immediate antibiotic prescribing. Delayed prescribing could reduce reconsultation rates and is unlikely to be associated with an increase in symptoms or illness duration, except in young children.
PROSPERO CRD42018079400.
评估社区呼吸道感染患者延迟使用抗生素对平均症状严重程度的总体影响,并确定任何可能改变这种影响的因素。
系统评价和个体患者数据荟萃分析。
Cochrane 对照试验中心注册库、Ovid Medline、Ovid Embase、EBSCO CINAHL Plus 和 Web of Science。
在社区环境中进行的随机对照试验和观察性队列研究,允许比较延迟与不使用抗生素、延迟与立即使用抗生素之间的差异。
主要结局是初始就诊后两到四天的平均症状严重程度,用七分制量表(从正常到最差)进行测量。次要结局包括初始就诊后疾病持续时间、导致住院或死亡的并发症、相同或恶化的疾病再次就诊以及基于李克特量表的患者满意度。
从 9 项随机对照试验和 4 项观察性研究中获得了数据,共纳入了 55682 名患者。与立即使用抗生素相比,延迟使用抗生素在随访时的症状严重程度(七分制量表)没有差异(调整平均差异-0.003,95%置信区间-0.12 至 0.11)或与不使用抗生素相比(0.02,-0.11 至 0.15)。与立即使用抗生素相比,给予延迟使用抗生素的患者症状持续时间略长(11.4 天比 10.9 天),但与不使用抗生素相比则相似。与不使用抗生素相比,延迟使用抗生素可降低导致住院或死亡的并发症发生率(比值比 0.62,95%置信区间 0.30 至 1.27)和延迟与立即使用抗生素(0.78,0.53 至 1.13)。与不使用抗生素相比,延迟使用抗生素可显著降低再次就诊率(比值比 0.72,95%置信区间 0.60 至 0.87)和提高患者满意度(调整平均差异 0.09,0.06 至 0.11)。与立即使用抗生素相比,延迟使用抗生素对儿童(年龄<5 岁)的随访症状严重程度略有升高(调整平均差异 0.10,95%置信区间 0.03 至 0.18),但在年龄较大的组中未发现症状加重。
对于大多数患者,包括高风险亚组患者,延迟使用抗生素是一种安全有效的策略。与不使用抗生素相比,延迟使用抗生素的症状持续时间相似,不太可能导致症状控制比立即使用抗生素差。延迟使用抗生素可能会降低再次就诊率,并且不太可能与症状或疾病持续时间的增加相关,除非在儿童中。
PROSPERO CRD42018079400。