Dipartimento di Neuroscienze, Riabilitazione, Oftalmologia, Genetica e Scienze Materno-Infantili (DINOGMI), University of Genoa, Largo Daneo 3, 16132 Genova, Italy.
IRCCS Ospedale Policlinico San Martino, Largo Rosanna Benzi 10, 16132 Genova, Italy.
Nutrients. 2021 Apr 7;13(4):1215. doi: 10.3390/nu13041215.
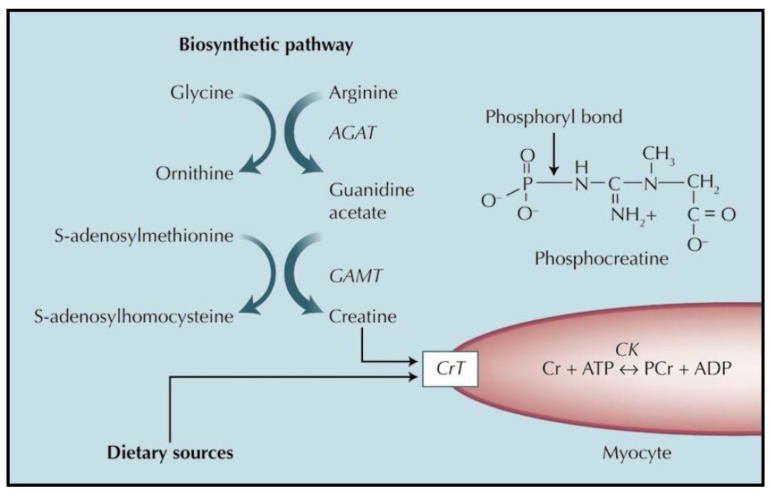
Creatine is a key player in heart contraction and energy metabolism. Creatine supplementation (throughout the paper, only supplementation with creatine monohydrate will be reviewed, as this is by far the most used and best-known way of supplementing creatine) increases creatine content even in the normal heart, and it is generally safe. In heart failure, creatine and phosphocreatine decrease because of decreased expression of the creatine transporter, and because phosphocreatine degrades to prevent adenosine triphosphate (ATP) exhaustion. This causes decreased contractility reserve of the myocardium and correlates with left ventricular ejection fraction, and it is a predictor of mortality. Thus, there is a strong rationale to supplement with creatine the failing heart. Pending additional trials, creatine supplementation in heart failure may be useful given data showing its effectiveness (1) against specific parameters of heart failure, and (2) against the decrease in muscle strength and endurance of heart failure patients. In heart ischemia, the majority of trials used phosphocreatine, whose mechanism of action is mostly unrelated to changes in the ergogenic creatine-phosphocreatine system. Nevertheless, preliminary data with creatine supplementation are encouraging, and warrant additional studies. Prevention of cardiac toxicity of the chemotherapy compounds anthracyclines is a novel field where creatine supplementation may also be useful. Creatine effectiveness in this case may be because anthracyclines reduce expression of the creatine transporter, and because of the pleiotropic antioxidant properties of creatine. Moreover, creatine may also reduce concomitant muscle damage by anthracyclines.
肌酸是心脏收缩和能量代谢的关键因素。肌酸补充(在整篇论文中,仅会回顾肌酸一水合物的补充,因为这是迄今为止使用最广泛和最知名的补充肌酸的方式)甚至可以增加正常心脏中的肌酸含量,而且通常是安全的。在心力衰竭中,由于肌酸转运体表达减少,以及由于磷酸肌酸降解以防止三磷酸腺苷(ATP)耗尽,肌酸和磷酸肌酸减少。这导致心肌收缩储备减少,与左心室射血分数相关,并且是死亡率的预测指标。因此,有充分的理由为衰竭的心脏补充肌酸。在等待进一步的试验结果的同时,鉴于补充肌酸显示出其对心力衰竭的有效性(1)针对心力衰竭的特定参数,以及(2)针对心力衰竭患者肌肉力量和耐力下降的有效性,补充肌酸可能对心力衰竭患者有益。在心肌缺血中,大多数试验使用磷酸肌酸,其作用机制主要与肌酸-磷酸肌酸系统的变化无关。然而,补充肌酸的初步数据令人鼓舞,值得进一步研究。预防化疗药物蒽环类药物的心脏毒性是肌酸补充可能也有用的一个新领域。在这种情况下,肌酸的有效性可能是因为蒽环类药物减少了肌酸转运体的表达,并且因为肌酸具有多种抗氧化特性。此外,肌酸还可以减少蒽环类药物引起的伴随性肌肉损伤。