On Jotaro, Natsumeda Manabu, Watanabe Jun, Saito Shoji, Kanemaru Yu, Abe Hideaki, Tsukamoto Yoshihiro, Okada Masayasu, Oishi Makoto, Yoshimura Junichi, Kakita Akiyoshi, Fujii Yukihiko
Department of Neurosurgery, Brain Research Institute, Niigata University, Niigata 951-8585, Japan.
Department of Pathology, Brain Research Institute, Niigata University, Niigata 951-8585, Japan.
Diagnostics (Basel). 2021 Apr 9;11(4):681. doi: 10.3390/diagnostics11040681.
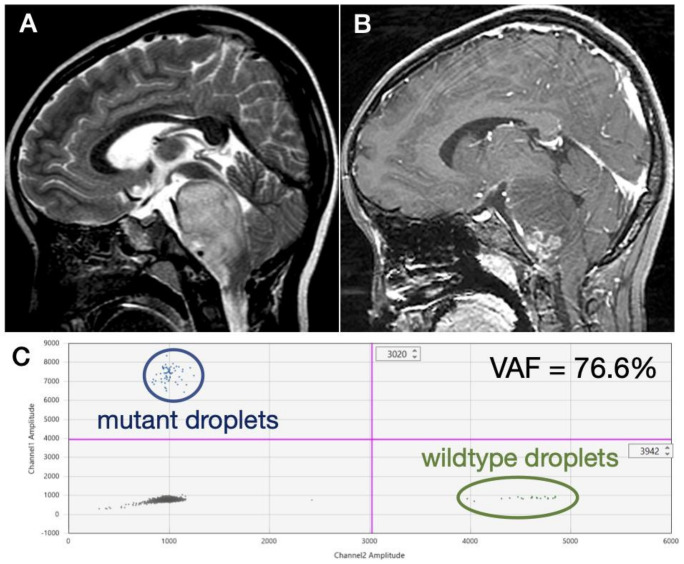
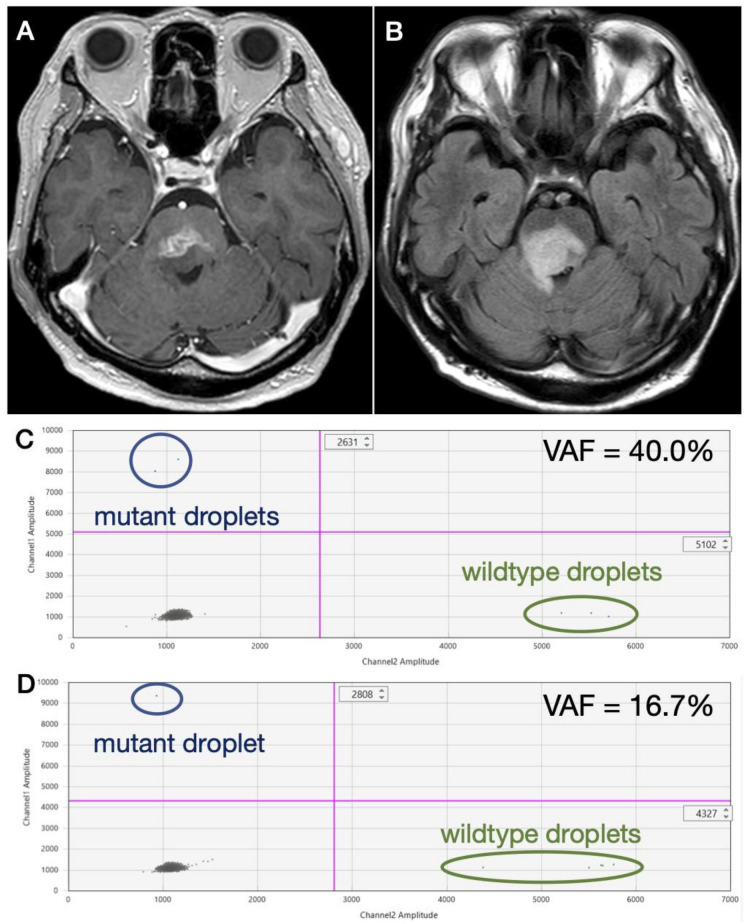
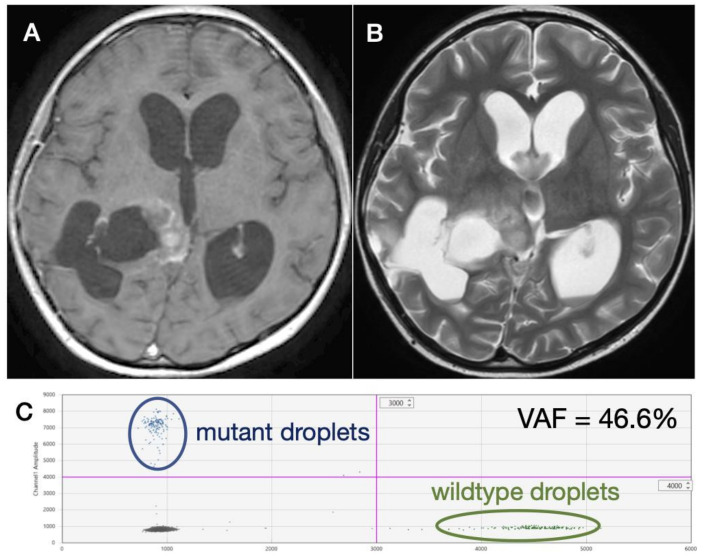
Recent studies have suggested the feasibility of detecting H3K27M mutations in the cerebrospinal fluid of diffuse midline glioma (DMG) patients. However, cerebrospinal fluid from patients in these studies were collected mainly during biopsy, ventriculo-peritoneal shunt procedures or postmortem. We assessed circulating tumor DNA (ctDNA) extracted from cerebrospinal fluid (CSF) and plasma in a series of 12 radiographically suspected and/or pathologically confirmed diffuse midline glioma patients and assessed for K27M mutation using digital droplet PCR. In 10 patients, CSF was obtained by lumbar puncture at presentation. A definitive detection of K27M mutation was achieved in only one case (10%); K27M mutation was suspected in three other cases (30%). K27M mutation was detected in two patients in CSF obtained by ventricular tap during a ventriculo-peritoneal shunt for obstructive hydrocephalus. Cases in which a definitive assessment was possible (definite K27M or definite wildtype) tended to be younger (median 7.5 years vs. 40.5 years; = 0.07) and have a higher concentration of CSF protein (median 123 mg/dL vs. 27.5 mg/dL; = 0.21) compared to nondefinite cases. Low proliferation and apoptotic rates seemed to be characteristics of DMG unfavorable for liquid biopsy. More advanced lesions with necrosis and evidence of dissemination were unlikely to be candidates for lumbar puncture due to the fear of exacerbating obstructive hydrocephalus. Methods to safely sample CSF and a more sensitive detection of ctDNA are necessary for reliable liquid biopsy of DMG at presentation.
近期研究表明,在弥漫性中线胶质瘤(DMG)患者的脑脊液中检测H3K27M突变具有可行性。然而,这些研究中患者的脑脊液主要是在活检、脑室 - 腹腔分流手术或尸检期间采集的。我们对12例影像学疑似和/或病理确诊的弥漫性中线胶质瘤患者的脑脊液(CSF)和血浆中提取的循环肿瘤DNA(ctDNA)进行了评估,并使用数字液滴PCR检测K27M突变。在10例患者中,就诊时通过腰椎穿刺获取脑脊液。仅在1例患者(10%)中实现了K27M突变的明确检测;在其他3例患者(30%)中疑似存在K27M突变。在因梗阻性脑积水进行脑室 - 腹腔分流期间通过脑室穿刺获取的脑脊液中,有2例患者检测到K27M突变。与非明确病例相比,能够进行明确评估(明确的K27M或明确的野生型)的病例往往更年轻(中位年龄7.5岁对40.5岁;P = 0.07),脑脊液蛋白浓度更高(中位值123mg/dL对27.5mg/dL;P = 0.21)。低增殖率和凋亡率似乎是不利于液体活检的DMG特征。由于担心加重梗阻性脑积水,伴有坏死和播散证据的更晚期病变不太可能成为腰椎穿刺的候选对象。对于DMG就诊时进行可靠的液体活检,安全采集脑脊液的方法和更灵敏的ctDNA检测是必要的。