Sakkas Andreas, Heil Sebastian, Kargus Steffen, Rebel Martin, Mischkowski Robert A, Thiele Oliver C
Department of Oral, Maxillofacial and Facial Plastic Surgery, Ludwigshafen Hospital, Ludwigshafen, Germany.
Department of Pathology, Ludwigshafen Hospital, Ludwigshafen, Germany.
GMS Interdiscip Plast Reconstr Surg DGPW. 2021 Apr 14;10:Doc03. doi: 10.3205/iprs000153. eCollection 2021.
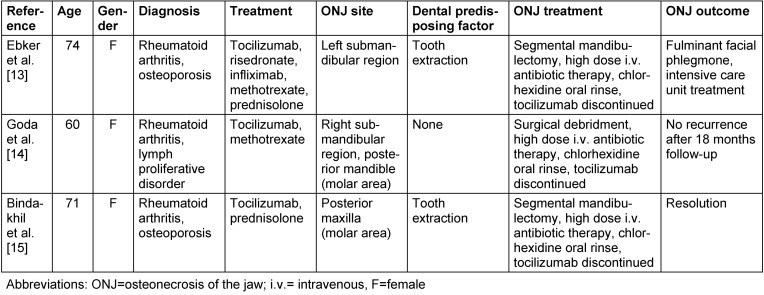
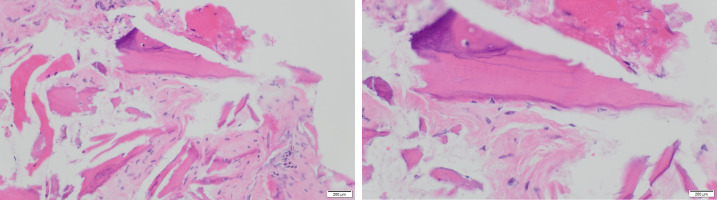
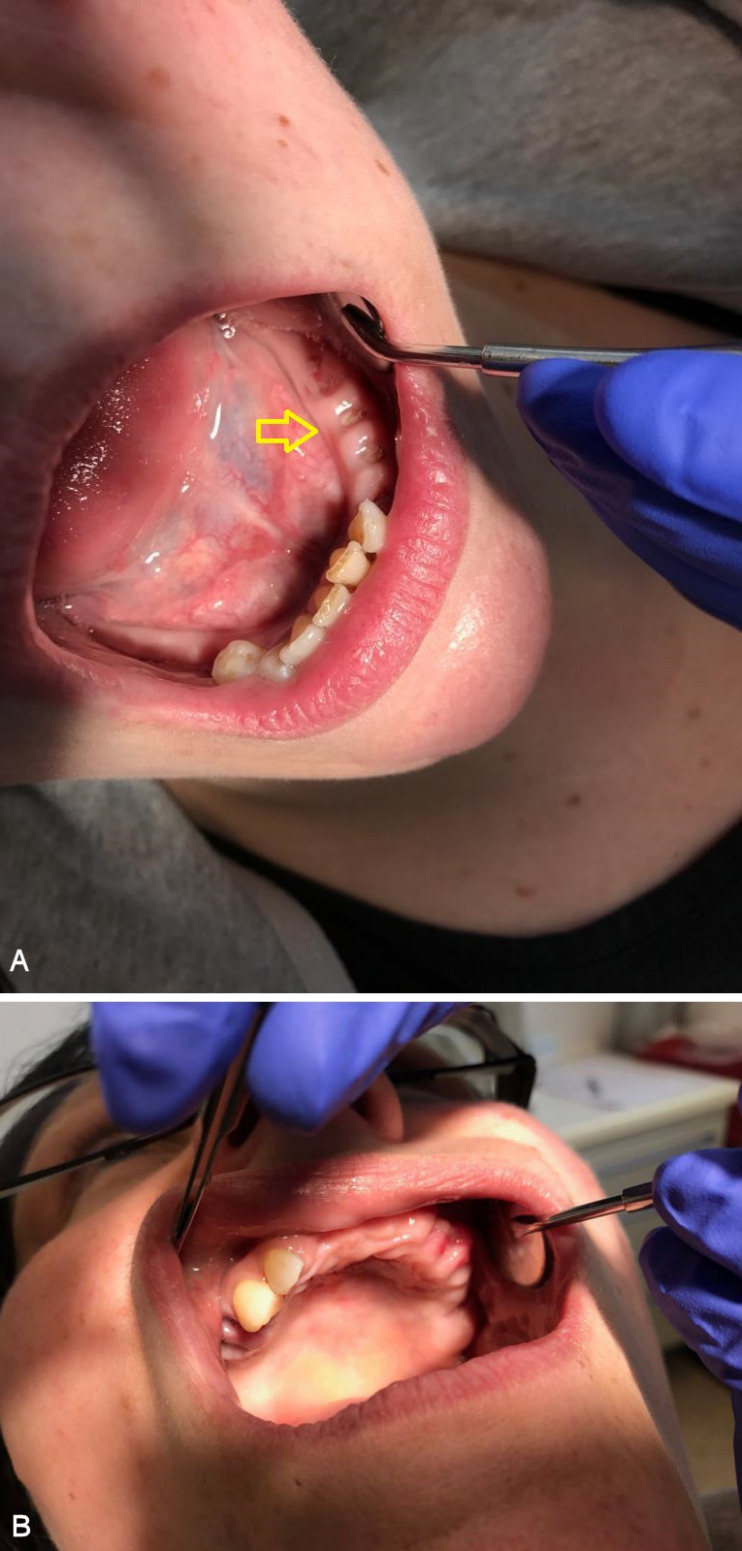
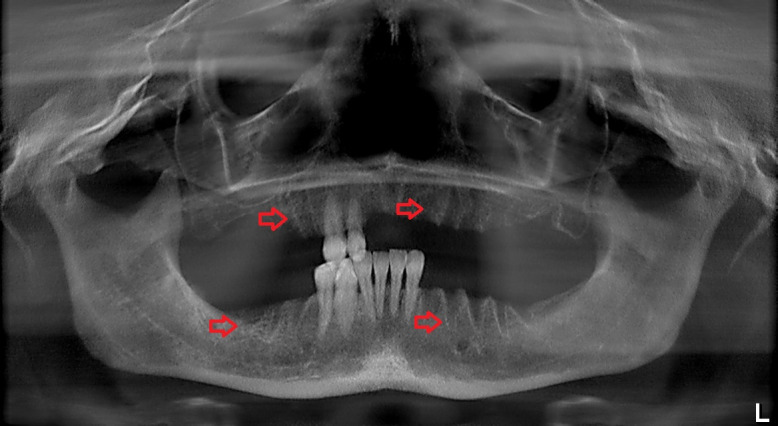
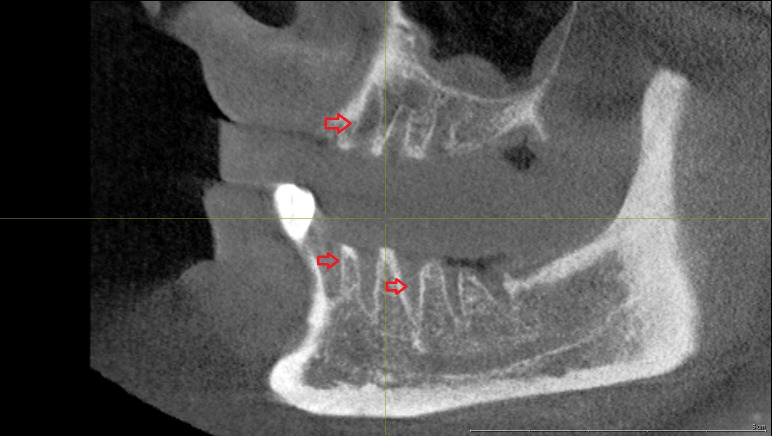
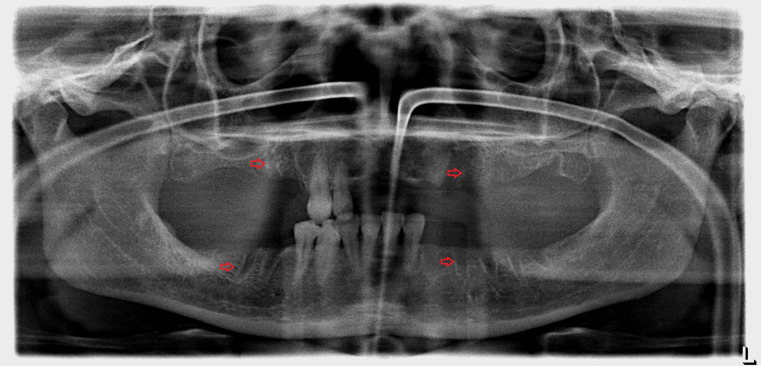
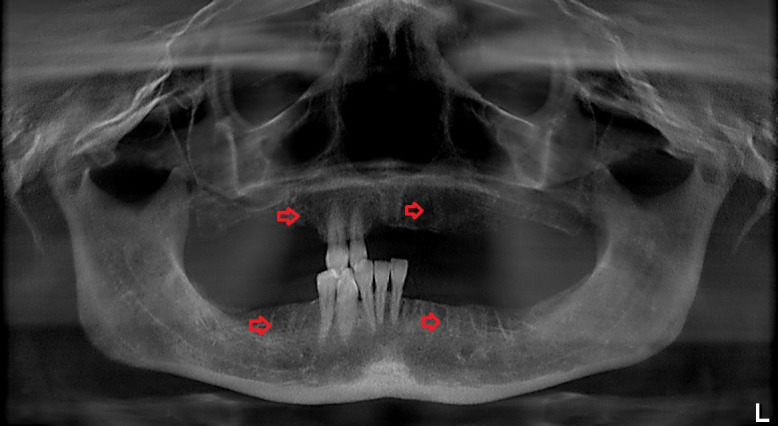
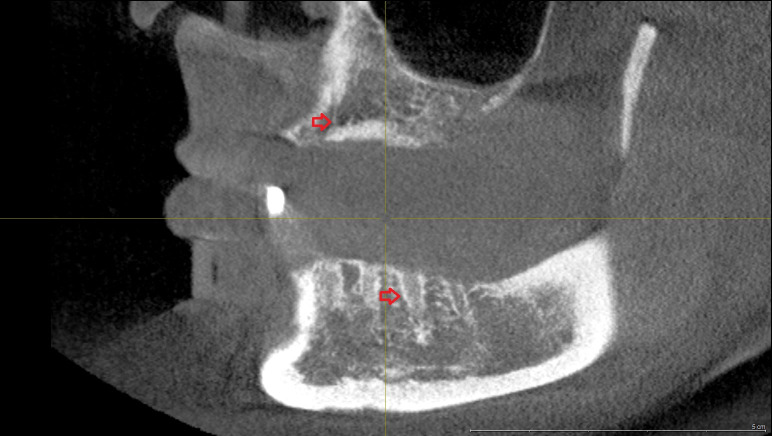
Medication-related osteonecrosis of the jaw (MRONJ) is a serious complication in patients receiving antiresorptive medication, such as bisphosphonates and denosumab, for different oncologic and non-oncologic diseases. Here, we report a case of MRONJ in a patient treated with tocilizumab, a humanized anti-interleukin-6 receptor antibody that effectively treats moderate to severe rheumatoid arthritis in adults. A 45-year-old female patient diagnosed with severe rheumatoid arthritis, who had been undergoing intravenous tocilizumab therapy for three years without history of bisphosphonate use, was referred to our department. Four weeks previously, several teeth in the maxilla and mandible were removed under local anesthesia by her dentist. Two weeks after the extractions, she felt pain in both jaws. We diagnosed wound dehiscence and delayed healing of the alveolar bone after the tooth extractions. Digital volume tomography showed persistent dry alveolar sockets. The patient underwent surgical debridement of necrotic bone, and intravenous antibiotics were administered in hospital. Five months later, wound dehiscence reoccurred in the same regions. Histopathological analysis of bone biopsies revealed a diagnosis of MRONJ. Four months later, wound dehiscence occurred in the left maxillary alveolar ridge, and local bone resection was performed under antibiotic treatment. Twenty-four months after the last surgery, wound dehiscence had healed completely without signs of recurrence. Osteomyelitis of the jaw in patients treated with tocilizumab has not been reported often. This case confirms the potential role of this interleukin-6 receptor inhibitor in the pathogenesis of MRONJ and shows that patients who receive tocilizumab with MRONJ-like symptoms should be closely monitored. The pathomechanism of MRONJ under tocilizumab therapy remains unclear, so dental practitioners, maxillofacial surgeons, and rheumatologists should look for signs of MRONJ in patients receiving tocilizumab to prevent MRONJ onset.
药物相关性颌骨坏死(MRONJ)是接受抗吸收药物(如双膦酸盐和地诺单抗)治疗不同肿瘤和非肿瘤疾病的患者中出现的一种严重并发症。在此,我们报告一例使用托珠单抗治疗的MRONJ病例,托珠单抗是一种人源化抗白细胞介素-6受体抗体,可有效治疗成人中度至重度类风湿性关节炎。一名45岁诊断为重度类风湿性关节炎的女性患者,接受静脉注射托珠单抗治疗三年,无使用双膦酸盐病史,被转诊至我科。四周前,她的牙医在局部麻醉下拔除了上颌和下颌的几颗牙齿。拔牙两周后,她感到双侧颌部疼痛。我们诊断为拔牙后牙槽骨伤口裂开和愈合延迟。数字容积断层扫描显示牙槽窝持续干燥。患者接受了坏死骨的手术清创,并在医院接受了静脉抗生素治疗。五个月后,同一区域再次出现伤口裂开。骨活检的组织病理学分析显示诊断为MRONJ。四个月后,左上颌牙槽嵴出现伤口裂开,并在抗生素治疗下进行了局部骨切除。最后一次手术后24个月,伤口裂开已完全愈合,无复发迹象。使用托珠单抗治疗的患者中颌骨骨髓炎的报道并不常见。该病例证实了这种白细胞介素-6受体抑制剂在MRONJ发病机制中的潜在作用,并表明出现MRONJ样症状的托珠单抗治疗患者应密切监测。托珠单抗治疗下MRONJ的发病机制仍不清楚,因此牙科医生、颌面外科医生和风湿病学家应在接受托珠单抗治疗的患者中寻找MRONJ的迹象,以预防MRONJ的发生。