The Population Health Research Institute, Hamilton Health Sciences, 237 Barton Street East, Hamilton, Ontario L8L 2X2, Canada.
The School of Rehabilitation Science, McMaster University, IAHS, Room 403, 1400 Main St. West, Hamilton, ON L8S 1C7, Canada.
Eur Heart J. 2021 Aug 17;42(31):2995-3007. doi: 10.1093/eurheartj/ehab225.
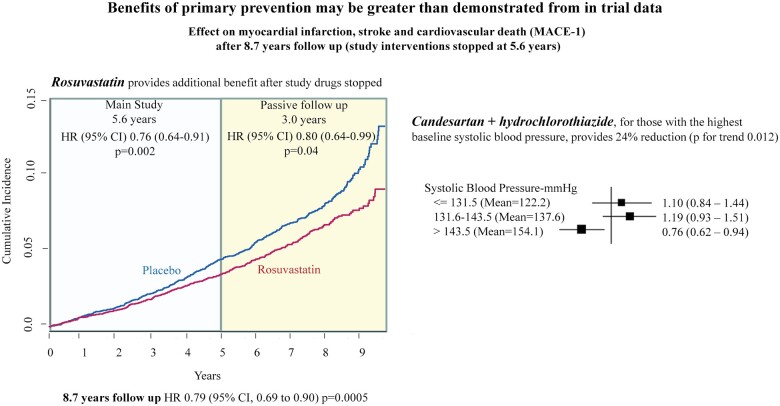
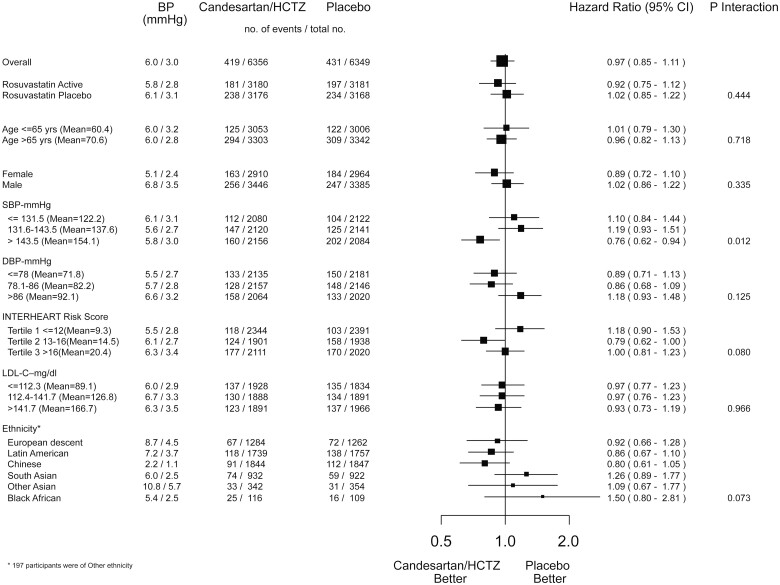
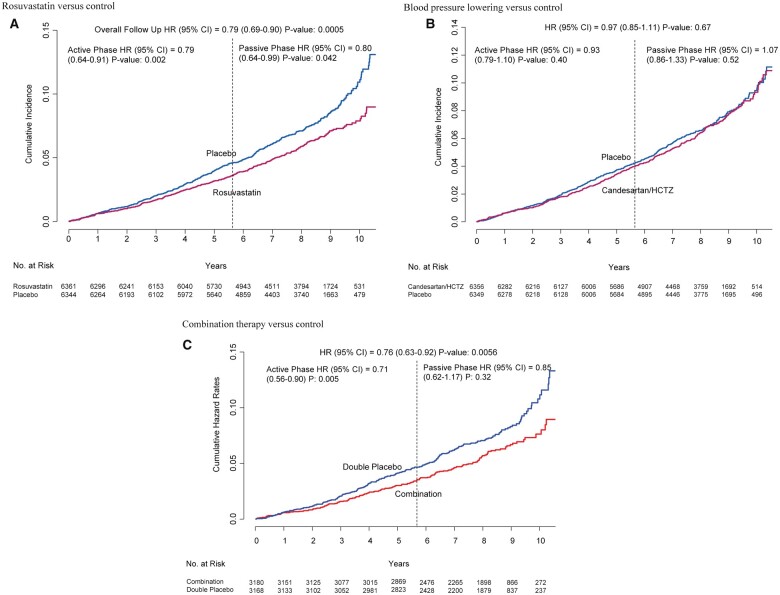
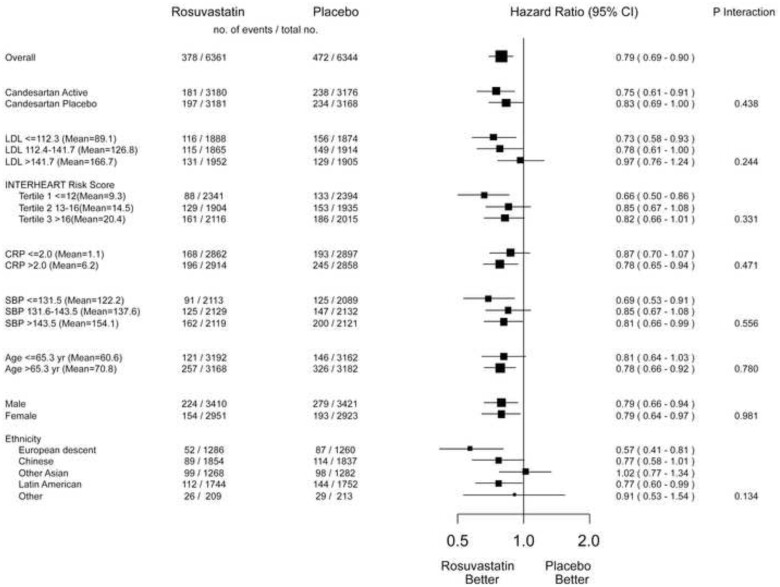
Rosuvastatin (10 mg per day) compared with placebo reduced major adverse cardiovascular (CV) events by 24% in 12 705 participants at intermediate CV risk after 5.6 years. There was no benefit of blood pressure (BP) lowering treatment in the overall group, but a reduction in events in the third of participants with elevated systolic BP. After cessation of all the trial medications, we examined whether the benefits observed during the active treatment phase were sustained, enhanced, or attenuated.
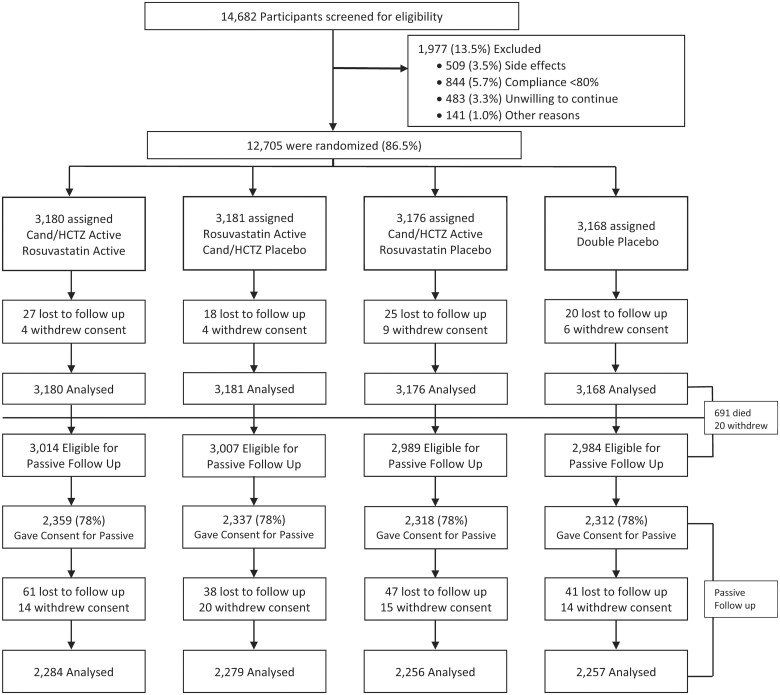
After the randomized treatment period (5.6 years), participants were invited to participate in 3.1 further years of observation (total 8.7 years). The first co-primary outcome for the entire length of follow-up was the composite of myocardial infarction, stroke, or CV death [major adverse cardiovascular event (MACE)-1], and the second was MACE-1 plus resuscitated cardiac arrest, heart failure, or coronary revascularization (MACE-2). In total, 9326 (78%) of 11 994 surviving Heart Outcomes Prevention Evaluation (HOPE)-3 subjects consented to participate in extended follow-up. During 3.1 years of post-trial observation (total follow-up of 8.7 years), participants originally randomized to rosuvastatin compared with placebo had a 20% additional reduction in MACE-1 [95% confidence interval (CI), 0.64-0.99] and a 17% additional reduction in MACE-2 (95% CI 0.68-1.01). Therefore, over the 8.7 years of follow-up, there was a 21% reduction in MACE-1 (95% CI 0.69-0.90, P = 0.005) and 21% reduction in MACE-2 (95% CI 0.69-0.89, P = 0.002). There was no benefit of BP lowering in the overall study either during the active or post-trial observation period, however, a 24% reduction in MACE-1 was observed over 8.7 years.
The CV benefits of rosuvastatin, and BP lowering in those with elevated systolic BP, compared with placebo continue to accrue for at least 3 years after cessation of randomized treatment in individuals without cardiovascular disease indicating a legacy effect.
NCT00468923.
在 12705 名具有中等心血管风险的参与者中,瑞舒伐他汀(每天 10 毫克)与安慰剂相比,可将主要不良心血管(CV)事件减少 24%,中位随访时间为 5.6 年。在整个研究人群中,降压治疗没有获益,但在收缩压升高的三分之一的参与者中,事件减少。在停止所有试验药物后,我们检查了在活性治疗阶段观察到的益处是否持续、增强或减弱。
在随机治疗期(5.6 年后),参与者被邀请参加 3.1 年的进一步观察(总随访 8.7 年)。整个随访期间的第一个主要复合终点是心肌梗死、卒中和心血管死亡的复合终点(主要不良心血管事件(MACE)-1),第二个主要复合终点是 MACE-1 加上复苏性心脏骤停、心力衰竭或冠状动脉血运重建(MACE-2)。共有 11994 名存活的心脏终点预防评估(HOPE)-3 受试者中的 9326 名(78%)同意参加扩展随访。在试验后 3.1 年的观察期间(总随访 8.7 年),与安慰剂相比,最初接受瑞舒伐他汀治疗的患者 MACE-1 额外降低 20%[95%置信区间(CI),0.64-0.99],MACE-2 额外降低 17%(95%CI,0.68-1.01)。因此,在 8.7 年的随访中,MACE-1 降低 21%(95%CI,0.69-0.90,P=0.005),MACE-2 降低 21%(95%CI,0.69-0.89,P=0.002)。无论是在活性治疗还是试验后观察期间,降压治疗都没有获益,然而,在 8.7 年的随访中,MACE-1 降低 24%。
与安慰剂相比,瑞舒伐他汀在无心血管疾病的个体中,在随机治疗停止后至少 3 年内,与血压降低相比,CV 获益仍在继续累积,表明存在遗留效应。
NCT00468923。