Division of Nursing, Midwifery and Social Work, School of Health Sciences, Faculty of Biology, Medicine and Health, University of Manchester, Manchester Academic Health Science Centre, Manchester, UK.
Division of Population Health, Health Services Research & Primary Care, Faculty of Biology, Medicine and Health, University of Manchester, Manchester, UK.
Cochrane Database Syst Rev. 2021 May 10;5(5):CD013620. doi: 10.1002/14651858.CD013620.pub2.
Pressure ulcers (also known as pressure injuries, pressure sores, decubitus ulcers and bed sores) are localised injuries to the skin or underlying soft tissue, or both, caused by unrelieved pressure, shear or friction. Alternating pressure (active) air surfaces are widely used with the aim of preventing pressure ulcers.
To assess the effects of alternating pressure (active) air surfaces (beds, mattresses or overlays) compared with any support surface on the incidence of pressure ulcers in any population in any setting.
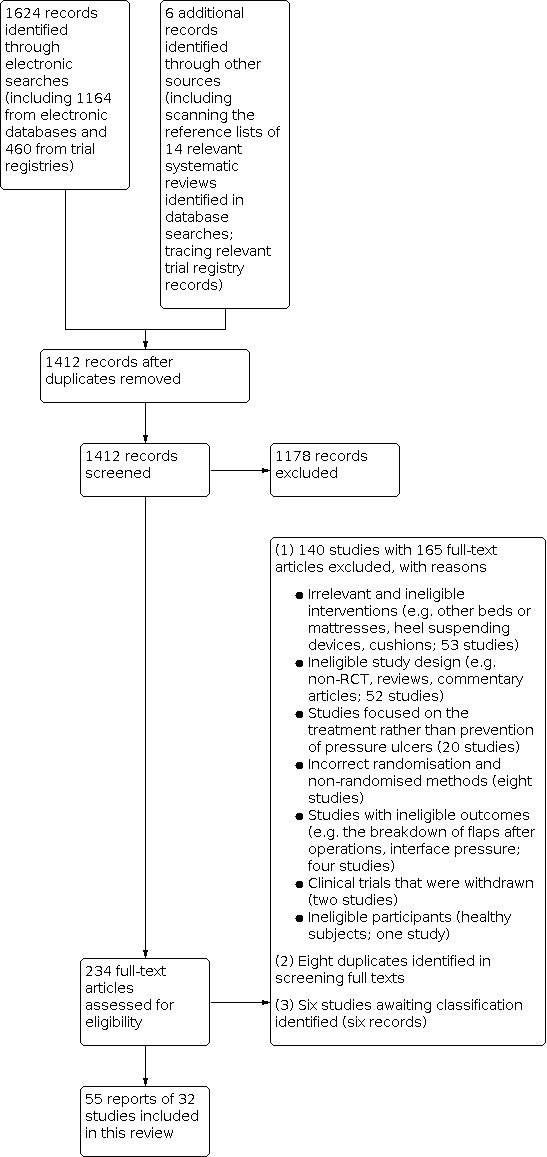
In November 2019, we searched the Cochrane Wounds Specialised Register; the Cochrane Central Register of Controlled Trials (CENTRAL); Ovid MEDLINE (including In-Process & Other Non-Indexed Citations); Ovid Embase and EBSCO CINAHL Plus. We also searched clinical trials registries for ongoing and unpublished studies, and scanned reference lists of relevant included studies as well as reviews, meta-analyses and health technology reports to identify additional studies. There were no restrictions with respect to language, date of publication or study setting.
We included randomised controlled trials that allocated participants of any age to alternating pressure (active) air beds, overlays or mattresses. Comparators were any beds, overlays or mattresses.
At least two review authors independently assessed studies using predetermined inclusion criteria. We carried out data extraction, 'Risk of bias' assessment using the Cochrane 'Risk of bias' tool, and the certainty of the evidence assessment according to Grading of Recommendations, Assessment, Development and Evaluations methodology.
We included 32 studies (9058 participants) in the review. Most studies were small (median study sample size: 83 participants). The average age of participants ranged from 37.2 to 87.0 years (median: 69.1 years). Participants were largely from acute care settings (including accident and emergency departments). We synthesised data for six comparisons in the review: alternating pressure (active) air surfaces versus: foam surfaces, reactive air surfaces, reactive water surfaces, reactive fibre surfaces, reactive gel surfaces used in the operating room followed by foam surfaces used on the ward bed, and another type of alternating pressure air surface. Of the 32 included studies, 25 (78.1%) presented findings which were considered at high overall risk of bias.
pressure ulcer incidence Alternating pressure (active) air surfaces may reduce the proportion of participants developing a new pressure ulcer compared with foam surfaces (risk ratio (RR) 0.63, 95% confidence interval (CI) 0.34 to 1.17; I = 63%; 4 studies, 2247 participants; low-certainty evidence). Alternating pressure (active) air surfaces applied on both operating tables and hospital beds may reduce the proportion of people developing a new pressure ulcer compared with reactive gel surfaces used on operating tables followed by foam surfaces applied on hospital beds (RR 0.22, 95% CI 0.06 to 0.76; I = 0%; 2 studies, 415 participants; low-certainty evidence). It is uncertain whether there is a difference in the proportion of people developing new pressure ulcers between alternating pressure (active) air surfaces and the following surfaces, as all these comparisons have very low-certainty evidence: (1) reactive water surfaces; (2) reactive fibre surfaces; and (3) reactive air surfaces. The comparisons between different types of alternating pressure air surfaces are presented narratively. Overall, all comparisons suggest little to no difference between these surfaces in pressure ulcer incidence (7 studies, 2833 participants; low-certainty evidence). Included studies have data on time to pressure ulcer incidence for three comparisons. When time to pressure ulcer development is considered using a hazard ratio (HR), it is uncertain whether there is a difference in the risk of developing new pressure ulcers, over 90 days' follow-up, between alternating pressure (active) air surfaces and foam surfaces (HR 0.41, 95% CI 0.10 to 1.64; I = 86%; 2 studies, 2105 participants; very low-certainty evidence). For the comparison with reactive air surfaces, there is low-certainty evidence that people treated with alternating pressure (active) air surfaces may have a higher risk of developing an incident pressure ulcer than those treated with reactive air surfaces over 14 days' follow-up (HR 2.25, 95% CI 1.05 to 4.83; 1 study, 308 participants). Neither of the two studies with time to ulcer incidence data suggested a difference in the risk of developing an incident pressure ulcer over 60 days' follow-up between different types of alternating pressure air surfaces. Secondary outcomes The included studies have data on (1) support-surface-associated patient comfort for comparisons involving foam surfaces, reactive air surfaces, reactive fibre surfaces and alternating pressure (active) air surfaces; (2) adverse events for comparisons involving foam surfaces, reactive gel surfaces and alternating pressure (active) air surfaces; and (3) health-related quality of life outcomes for the comparison involving foam surfaces. However, all these outcomes and comparisons have low or very low-certainty evidence and it is uncertain whether there are any differences in these outcomes. Included studies have data on cost effectiveness for two comparisons. Moderate-certainty evidence suggests that alternating pressure (active) air surfaces are probably more cost-effective than foam surfaces (1 study, 2029 participants) and that alternating pressure (active) air mattresses are probably more cost-effective than overlay versions of this technology for people in acute care settings (1 study, 1971 participants).
AUTHORS' CONCLUSIONS: Current evidence is uncertain about the difference in pressure ulcer incidence between using alternating pressure (active) air surfaces and other surfaces (reactive water surfaces, reactive fibre surfaces and reactive air surfaces). Alternating pressure (active) air surfaces may reduce pressure ulcer risk compared with foam surfaces and reactive gel surfaces used on operating tables followed by foam surfaces applied on hospital beds. People using alternating pressure (active) air surfaces may be more likely to develop new pressure ulcers over 14 days' follow-up than those treated with reactive air surfaces in the nursing home setting; but as the result is sensitive to the choice of outcome measure it should be interpreted cautiously. Alternating pressure (active) air surfaces are probably more cost-effective than reactive foam surfaces in preventing new pressure ulcers. Future studies should include time-to-event outcomes and assessment of adverse events and trial-level cost-effectiveness. Further review using network meta-analysis will add to the findings reported here.
压疮(也称为压力性损伤、压力性溃疡、褥疮和床疮)是由于持续的压力、剪切力或摩擦力导致的皮肤或皮下软组织的局部损伤。交替压力(主动)空气表面广泛用于预防压疮。
评估交替压力(主动)空气表面(床、床垫或覆盖物)与任何支撑面在任何人群和任何环境中预防压疮的效果。
2019 年 11 月,我们检索了 Cochrane 伤口专业注册库;Cochrane 对照试验中心注册库(CENTRAL);Ovid MEDLINE(包括正在进行的和其他非索引引文);Ovid Embase 和 EBSCO CINAHL Plus。我们还检索了正在进行和未发表研究的临床试验登记处,并对相关纳入研究的参考文献列表以及综述、荟萃分析和卫生技术报告进行了扫描,以确定其他研究。对语言、发表日期或研究环境没有任何限制。
我们纳入了将任何年龄的参与者随机分配到交替压力(主动)空气床、覆盖物或床垫的随机对照试验。对照是任何床、覆盖物或床垫。
至少两名综述作者独立使用预定的纳入标准评估研究。我们进行了数据提取、使用 Cochrane“风险偏倚”工具进行“风险偏倚”评估,并根据推荐评估、制定和评估(GRADE)方法评估证据的确定性。
我们纳入了 32 项研究(9058 名参与者)。大多数研究规模较小(中位数研究样本量:83 名参与者)。参与者的平均年龄范围从 37.2 岁到 87.0 岁(中位数:69.1 岁)。参与者主要来自急性护理环境(包括事故和急救部门)。我们对综述中的六项比较进行了数据综合:交替压力(主动)空气表面与:泡沫表面、反应性空气表面、反应性水表面、反应性纤维表面、反应性凝胶表面(用于手术室)后再使用泡沫表面(用于病房床上)和另一种类型的交替压力空气表面。在纳入的 32 项研究中,25 项(78.1%)研究的结果被认为整体存在高偏倚风险。
压疮发生率 与泡沫表面相比,交替压力(主动)空气表面可能降低新发压疮的比例(风险比 (RR) 0.63,95%置信区间 (CI) 0.34 至 1.17;I = 63%;4 项研究,2247 名参与者;低质量证据)。在手术室使用的反应性凝胶表面和在病房床上使用的泡沫表面之后,交替压力(主动)空气表面可能降低新发压疮的比例与反应性纤维表面(RR 0.22,95%CI 0.06 至 0.76;I = 0%;2 项研究,415 名参与者;低质量证据)。不确定与以下表面相比,交替压力(主动)空气表面是否存在新发压疮比例的差异,因为所有这些比较都具有非常低质量的证据:(1)反应性水表面;(2)反应性纤维表面;和(3)反应性空气表面。不同类型的交替压力空气表面之间的比较是通过叙述来呈现的。总体而言,所有比较都表明这些表面在压疮发生率方面几乎没有差异(7 项研究,2833 名参与者;低质量证据)。纳入的研究有关于三种比较的压疮发生时间的数据。当使用危险比(HR)考虑到压疮发展的时间时,不确定在 90 天的随访中,交替压力(主动)空气表面与泡沫表面相比,新发压疮的风险是否存在差异(HR 0.41,95%CI 0.10 至 1.64;I = 86%;2 项研究,2105 名参与者;极低质量证据)。对于与反应性空气表面的比较,有低质量证据表明,与反应性空气表面相比,接受交替压力(主动)空气表面治疗的人在 14 天的随访中更有可能发生新发压疮(HR 2.25,95%CI 1.05 至 4.83;1 项研究,308 名参与者)。没有一项有压疮发生时间数据的两项研究表明,在 60 天的随访中,不同类型的交替压力空气表面之间发生新发压疮的风险存在差异。次要结局 纳入的研究有关于(1)比较涉及泡沫表面、反应性空气表面、反应性纤维表面和交替压力(主动)空气表面时的支持面相关患者舒适度的结果;(2)比较涉及泡沫表面、反应性凝胶表面和交替压力(主动)空气表面时的不良事件结果;和(3)比较涉及泡沫表面时的健康相关生活质量结果。然而,所有这些结果和比较都具有低或非常低质量的证据,不确定这些结果是否存在差异。纳入的研究有关于两种比较的成本效益的数据。中等质量证据表明,与泡沫表面相比,交替压力(主动)空气表面可能更具成本效益(1 项研究,2029 名参与者),并且在急性护理环境中,交替压力(主动)空气床垫可能比该技术的覆盖版本更具成本效益(1 项研究,1971 名参与者)。
目前的证据不确定使用交替压力(主动)空气表面与其他表面(反应性水表面、反应性纤维表面和反应性空气表面)在压疮发生率方面的差异。与泡沫表面相比,交替压力(主动)空气表面可能降低压疮风险,与在手术室使用的反应性凝胶表面和在病房床上使用的泡沫表面相比。在疗养院环境中,使用交替压力(主动)空气表面的人在 14 天的随访中比使用反应性空气表面的人更有可能发生新的压疮;但由于结果对结局测量的选择敏感,因此应谨慎解释。与反应性泡沫表面相比,交替压力(主动)空气表面在预防新发压疮方面可能更具成本效益。未来的研究应包括时间到事件结局和不良事件评估以及试验水平的成本效益。进一步使用网络荟萃分析的审查将增加本报告中报告的结果。