Division of Infectious Diseases, Duke University Medical Center, Durham, North Carolina.
Duke Center for Antimicrobial Stewardship and Infection Prevention, Durham, North Carolina.
JAMA Netw Open. 2021 May 3;4(5):e219820. doi: 10.1001/jamanetworkopen.2021.9820.
Penicillin allergies are frequently mislabeled, which may contribute to use of less-preferred alternative antibiotics.
To evaluate a pharmacist-led allergy assessment program's association with antimicrobial use and clinical outcomes.
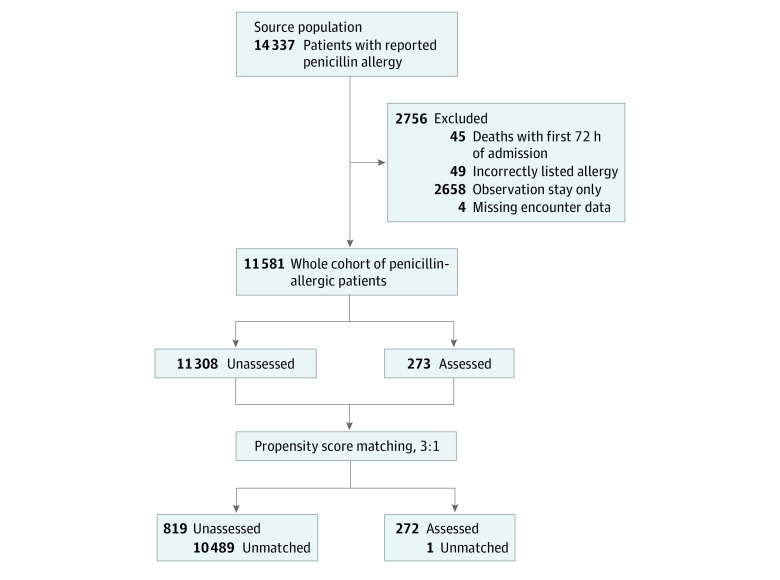
DESIGN, SETTING, AND PARTICIPANTS: A pharmacist-led allergy assessment program was launched in 2 phases (June 1, 2015, and November 2, 2016) at a single-center tertiary referral hospital. The longitudinal cross-sectional study included all study period adult admissions; hospitalwide outcomes were assessed by segmented regression. Individual outcomes were assessed within an embedded propensity score-matched case-control study of inpatients undergoing comprehensive allergy assessment following self-report of penicillin allergy. Analysis occurred from March 1, 2020, to February 29, 2020.
The longitudinal study analyzed hospital-level outcomes over 3 periods: preintervention (15 months), phase 1 (structured allergy history alone, 16 months), and phase 2 (comprehensive assessment including penicillin skin testing, 52 months). The case-control study defined cases as individuals undergoing comprehensive allergy assessment.
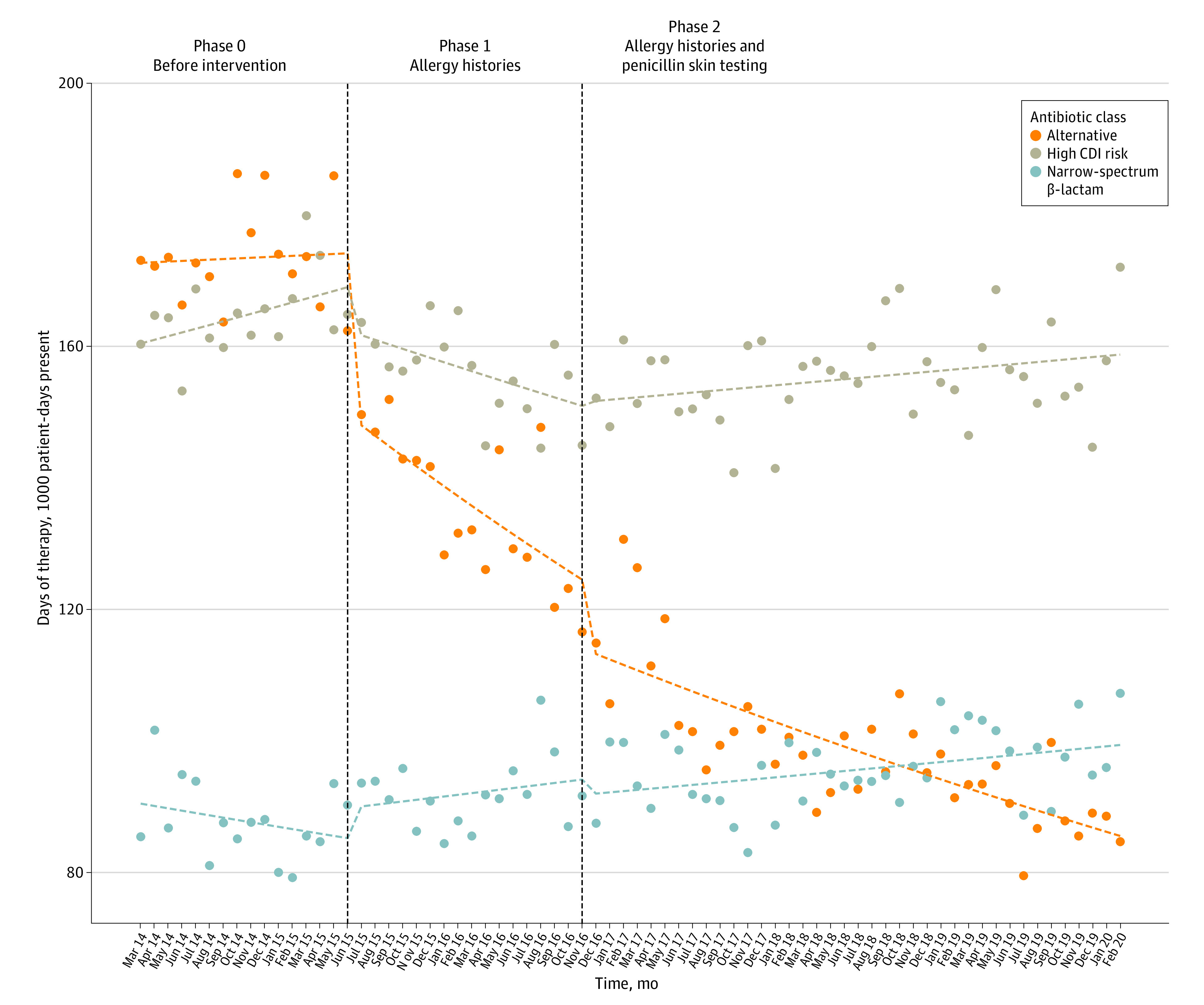
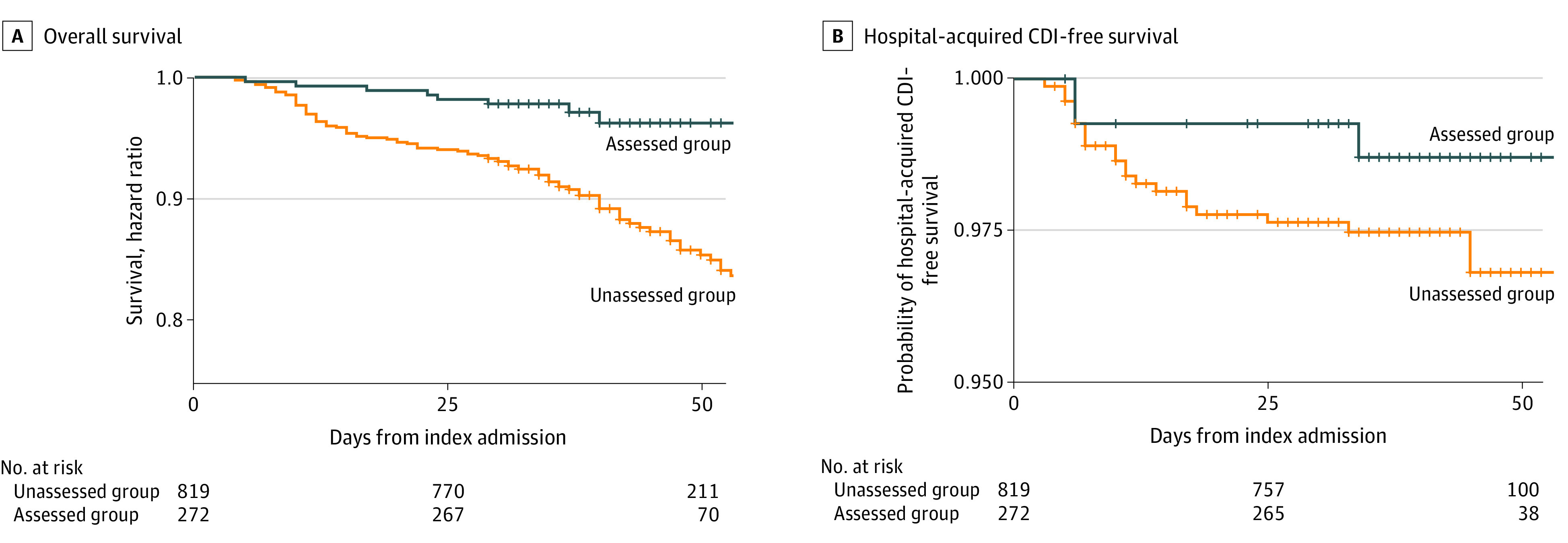
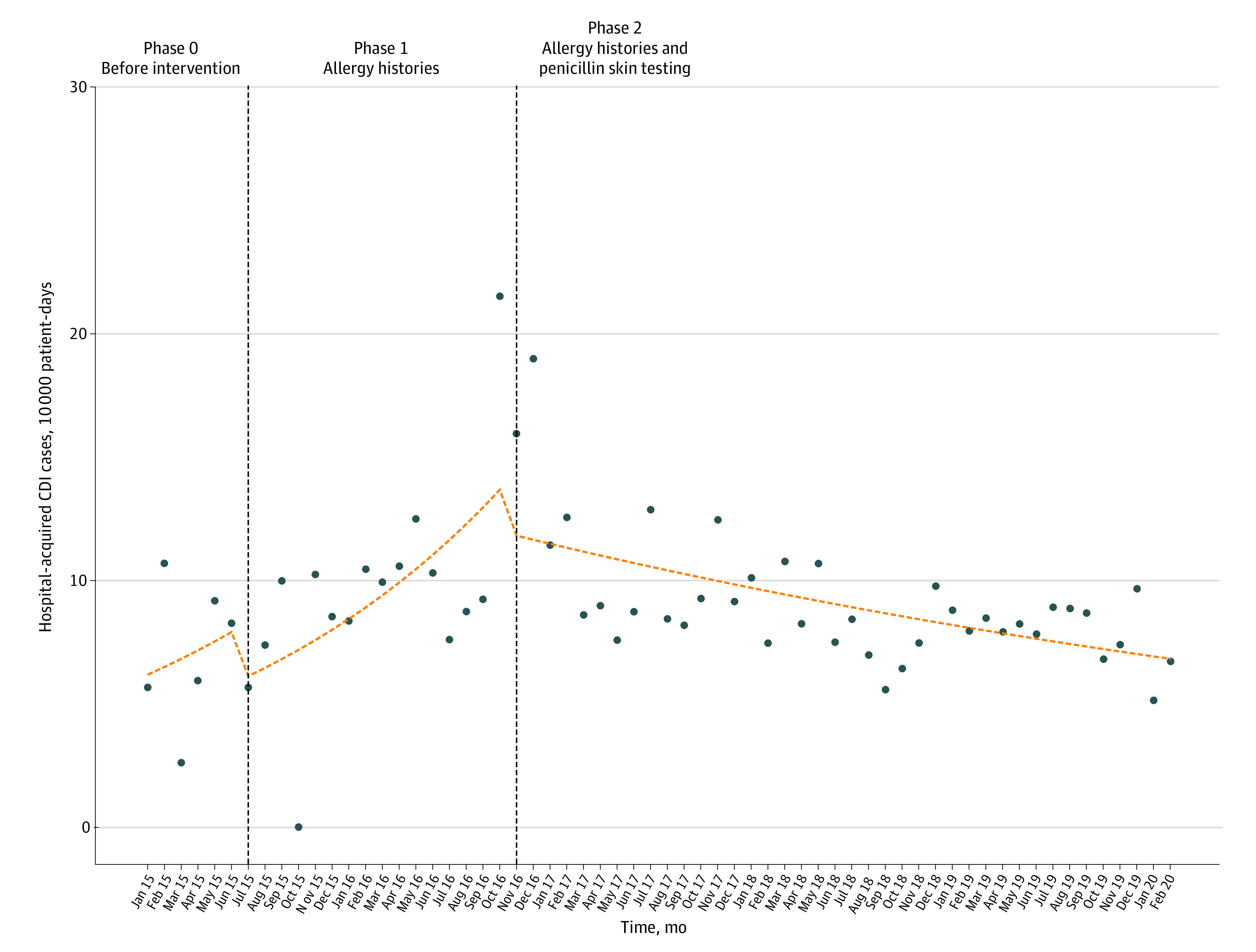
Hospital-level outcomes included antibiotic days of therapy per 1000 patient-days and hospital-acquired Clostridioides difficile infection (CDI) incidence per 10 000 patient-days. Individual outcomes included antibiotic selection, overall survival, and CDI-free survival.
Longitudinal analysis spanned 2014-2020 (median admissions, 46 416 per year; interquartile range [IQR], 46 001-50 091 per year). Hospitalwide, allergy histories were temporally associated with decreased use of nonpenicillin alternative antibiotics (rate ratio, 0.87; 95% CI, 0.79-0.97) and high-CDI-risk antibiotics (rate ratio, 0.91; 95% CI, 0.85-0.98). Penicillin skin testing was temporally associated with lower hospital-acquired CDI rates (rate ratio, 0.61; 95% CI, 0.43-0.86). The embedded case-control study included 272 cases and 819 controls. Median age was 63 years (interquartile range, 51-73 years), 553 (50.7%) patients were women, and 229 (21.0%) patients were Black. Allergy-assessed patients were less likely to receive high-CDI-risk antibiotics at discharge (odds ratio, 0.66; 95% CI, 0.44-0.98). Estimated reductions in mortality (hazard ratio, 0.77; 95% CI, 0.55-1.07) and hospital-acquired CDI risk (hazard ratio, 0.53; 95% CI, 0.18-1.55) were not statistically significant.
Pharmacist-led allergy assessments may be associated with reduced high-CDI-risk antibiotic use at both hospitalwide and individual levels. Although individual reductions in mortality and CDI risk did not achieve significance, divergence of survival curves suggest longer-term benefits of allergy delabeling warrant future study.
青霉素过敏经常被错误标记,这可能导致使用不太理想的替代抗生素。
评估药师主导的过敏评估计划与抗菌药物使用和临床结果的关系。
设计、地点和参与者:一项药师主导的过敏评估计划分两个阶段(2015 年 6 月 1 日和 2016 年 11 月 2 日)在一家单中心三级转诊医院启动。这项纵向的病例对照研究包括所有研究期间的成年住院患者;通过分段回归评估医院范围的结果。个体结果在一项嵌入式倾向评分匹配的病例对照研究中进行评估,该研究对自我报告青霉素过敏的住院患者进行了全面过敏评估。分析于 2020 年 3 月 1 日至 2020 年 2 月 29 日进行。
纵向研究在三个时期分析了医院层面的结果:干预前(15 个月)、第 1 阶段(仅进行结构化过敏史评估,16 个月)和第 2 阶段(进行全面评估,包括青霉素皮试,52 个月)。病例对照研究将接受全面过敏评估的个体定义为病例。
医院层面的结果包括每 1000 名患者-天的抗生素治疗天数和每 10000 名患者-天的医院获得性艰难梭菌感染(CDI)发生率。个体结果包括抗生素选择、总生存率和 CDI 无复发生存率。
纵向分析跨越了 2014 年至 2020 年(中位数入院人数为每年 46416 人;四分位间距[IQR]为每年 46001 人至 50091 人)。在医院范围内,过敏史与非青霉素替代抗生素的使用减少有关(比率比,0.87;95%CI,0.79-0.97)和高 CDI 风险抗生素(比率比,0.91;95%CI,0.85-0.98)。青霉素皮试与较低的医院获得性 CDI 发生率有关(比率比,0.61;95%CI,0.43-0.86)。嵌入式病例对照研究包括 272 例病例和 819 例对照。中位年龄为 63 岁(IQR,51-73 岁),553 名(50.7%)患者为女性,229 名(21.0%)患者为黑人。接受过敏评估的患者在出院时更不可能使用高 CDI 风险的抗生素(比值比,0.66;95%CI,0.44-0.98)。估计死亡率(风险比,0.77;95%CI,0.55-1.07)和医院获得性 CDI 风险(风险比,0.53;95%CI,0.18-1.55)降低的结果没有统计学意义。
药师主导的过敏评估可能与医院层面和个体层面的高 CDI 风险抗生素使用减少有关。尽管个体死亡率和 CDI 风险的降低没有达到统计学意义,但生存曲线的差异表明,过敏标记的消除带来的长期获益值得进一步研究。