Center for Cardiovascular Medicine, Interdisciplinary Center for Sleep Medicine, Charité-Universitätsmedizin Berlin, Luisenstraße 13, 10117, Berlin, Germany.
Sleep and Ventilation Center Blaubeuren, Lung Center Ulm, Ulm, Germany.
Sleep Breath. 2022 Mar;26(1):269-277. doi: 10.1007/s11325-021-02371-7. Epub 2021 May 15.
Diagnosis and treatment of obstructive sleep apnea are traditionally performed in sleep laboratories with polysomnography (PSG) and are associated with significant waiting times for patients and high cost. We investigated if initiation of auto-titrating CPAP (APAP) treatment at home in patients with obstructive sleep apnea (OSA) and subsequent telemonitoring by a homecare provider would be non-inferior to in-lab management with diagnostic PSG, subsequent in-lab APAP initiation, and standard follow-up regarding compliance and disease-specific quality of life.
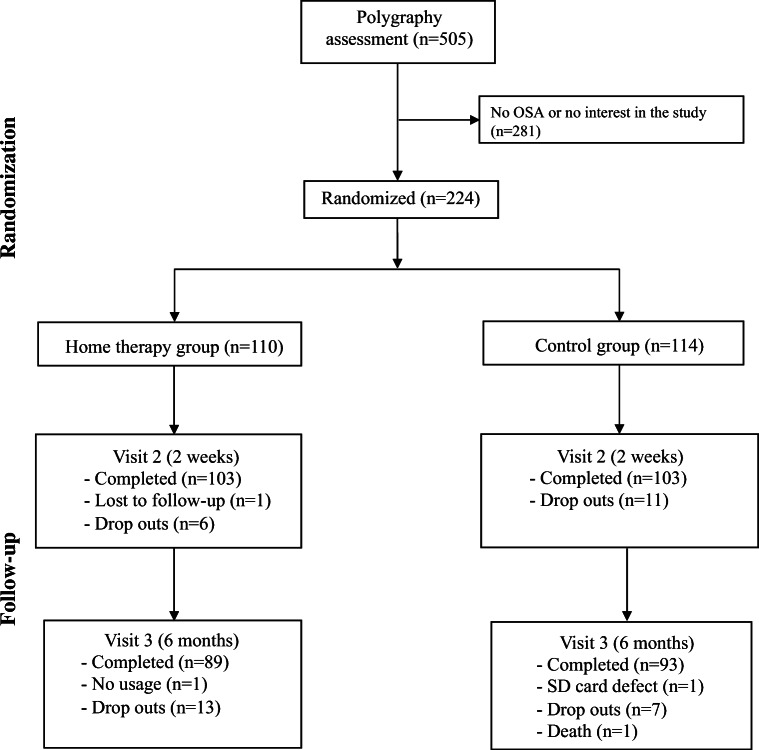
This randomized, open-label, single-center study was conducted in Germany. Screening occurred between December 2013 and November 2015. Eligible patients with moderate-to-severe OSA documented by polygraphy (PG) were randomized to home management or standard care. All patients were managed by certified sleep physicians. The home management group received APAP therapy at home, followed by telemonitoring. The control group received a diagnostic PSG, followed by therapy initiation in the sleep laboratory. The primary endpoint was therapy compliance, measured as average APAP usage after 6 months.
The intention-to-treat population (ITT) included 224 patients (110 home therapy, 114 controls); the per-protocol population (PP) included 182 patients with 6-month device usage data (89 home therapy, 93 controls). In the PP analysis, mean APAP usage at 6 months was not different in the home therapy and control groups (4.38 ± 2.04 vs. 4.32 ± 2.28, p = 0.845). The pre-specified non-inferiority margin (NIM) of 0.3 h/day was not achieved (p = 0.130); statistical significance was achieved in a post hoc analysis when NIM was set at 0.5 h/day (p < 0.05). Time to APAP initiation was significantly shorter in the home therapy group (7.6 ± 7.2 vs. 46.1 ± 23.8 days; p < 0.0001).
Use of a home-based telemonitoring strategy for initiation of APAP in selected patients with OSA managed by sleep physicians is feasible, appears to be non-inferior to standard sleep laboratory procedures, and facilitates faster access to therapy.
阻塞性睡眠呼吸暂停的诊断和治疗传统上是在睡眠实验室进行的,需要进行多导睡眠图(PSG)检查,这会导致患者等待时间长,费用高。我们研究了在家中使用自动滴定持续气道正压通气(APAP)治疗(APAP)治疗阻塞性睡眠呼吸暂停(OSA)患者,随后由家庭护理提供者进行远程监测,与在实验室进行诊断性 PSG 检查、随后在实验室中进行 APAP 启动以及标准随访以评估依从性和疾病特异性生活质量,是否具有非劣效性。
这是一项在德国进行的随机、开放标签、单中心研究。筛选于 2013 年 12 月至 2015 年 11 月进行。通过多导睡眠图(PG)记录到中度至重度 OSA 的合格患者被随机分配至家庭管理或标准护理组。所有患者均由经过认证的睡眠医师进行管理。家庭管理组在家中接受 APAP 治疗,随后进行远程监测。对照组接受诊断性 PSG 检查,随后在睡眠实验室中开始治疗。主要终点是治疗依从性,以 6 个月后的平均 APAP 使用量来衡量。
意向治疗人群(ITT)包括 224 例患者(家庭治疗组 110 例,对照组 114 例);符合方案人群(PP)包括 182 例有 6 个月设备使用数据的患者(家庭治疗组 89 例,对照组 93 例)。在 PP 分析中,家庭治疗组和对照组在 6 个月时的平均 APAP 使用量无差异(4.38±2.04 与 4.32±2.28,p=0.845)。未达到预定的非劣效性边界(NIM)0.3 小时/天(p=0.130);当 NIM 设置为 0.5 小时/天时,在事后分析中达到了统计学意义(p<0.05)。家庭治疗组的 APAP 启动时间明显缩短(7.6±7.2 与 46.1±23.8 天;p<0.0001)。
在睡眠医师管理的 OSA 患者中,使用基于家庭的远程监测策略启动 APAP 是可行的,似乎不劣于标准睡眠实验室程序,并且可以更快地获得治疗。