Green Mark A, García-Fiñana Marta, Barr Ben, Burnside Girvan, Cheyne Christopher P, Hughes David, Ashton Matthew, Sheard Sally, Buchan Iain E
Senior Lecturer in Health Geography, Department of Geography & Planning, University of Liverpool, Liverpool, UK.
Professor of Health Data Science, Department of Health Data Science, University of Liverpool, Liverpool, UK.
Lancet Reg Health Eur. 2021 Jul;6:100107. doi: 10.1016/j.lanepe.2021.100107. Epub 2021 May 12.
Large-scale asymptomatic testing of communities in Liverpool (UK) for SARS-CoV-2 was used as a public health tool for containing COVID-19. The aim of the study is to explore social and spatial inequalities in uptake and case-detection of rapid lateral flow SARS-CoV-2 antigen tests (LFTs) offered to people without symptoms of COVID-19.
Linked pseudonymised records for asymptomatic residents in Liverpool who received a LFT for COVID-19 between 6th November 2020 to 31st January 2021 were accessed using the Combined Intelligence for Population Health Action resource. Bayesian Hierarchical Poisson Besag, York, and Mollié models were used to estimate ecological associations for uptake and positivity of testing.
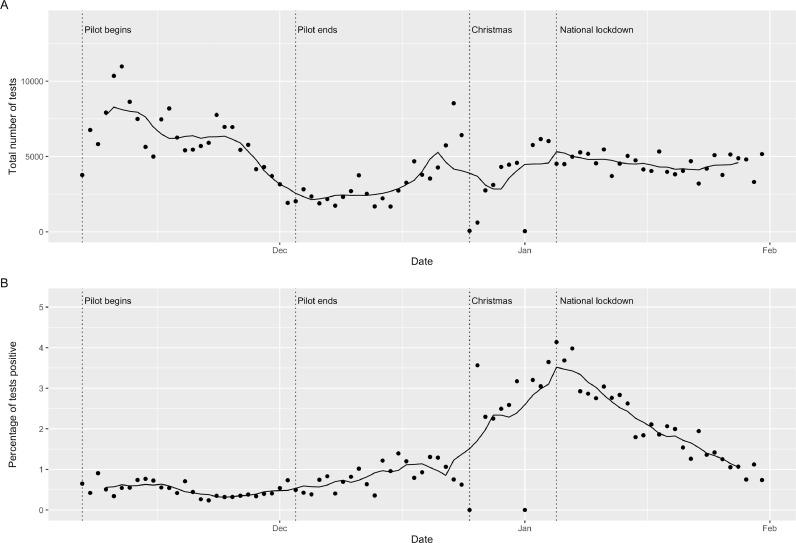
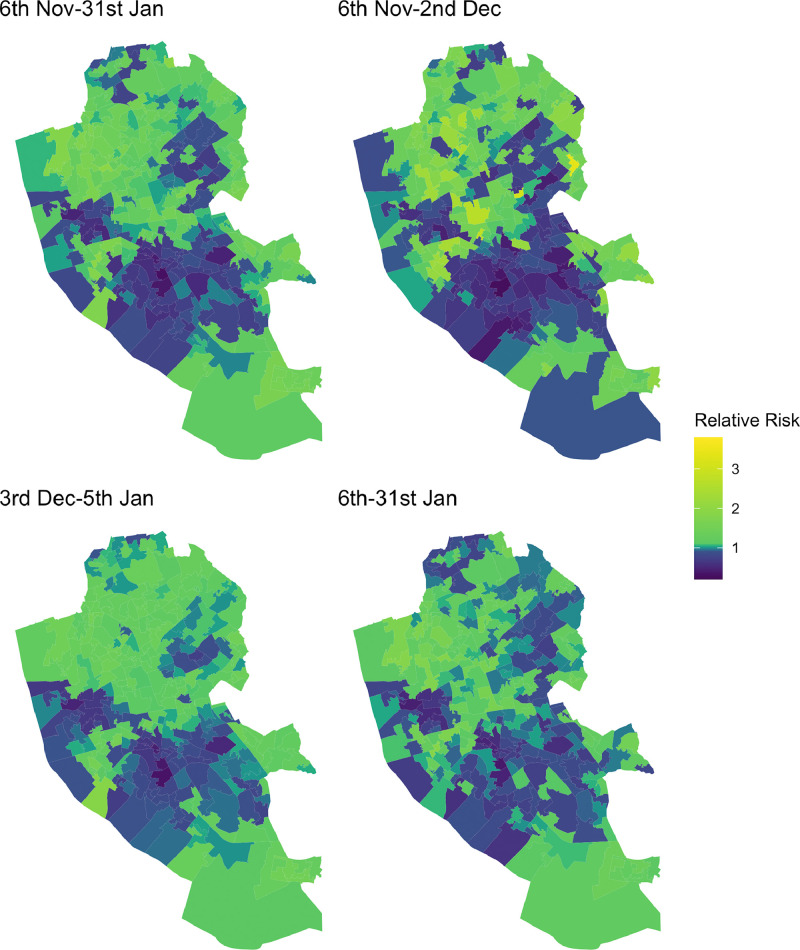
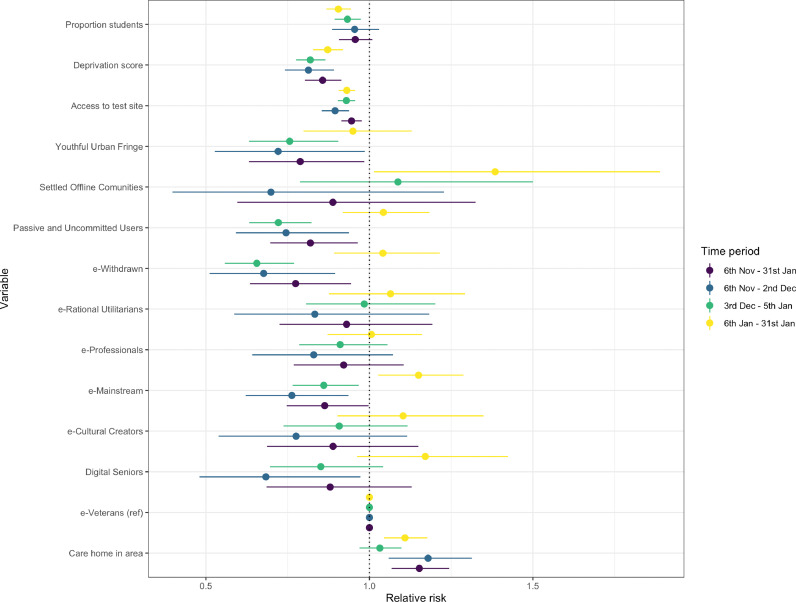
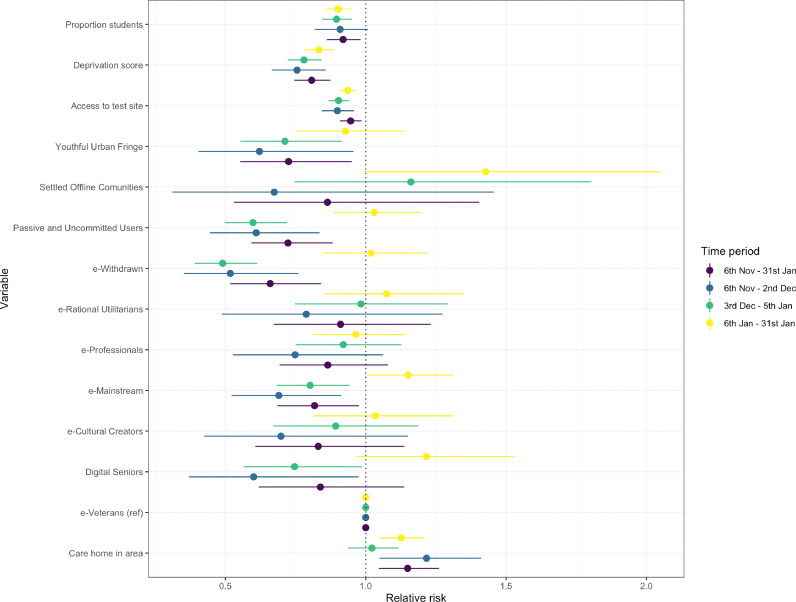
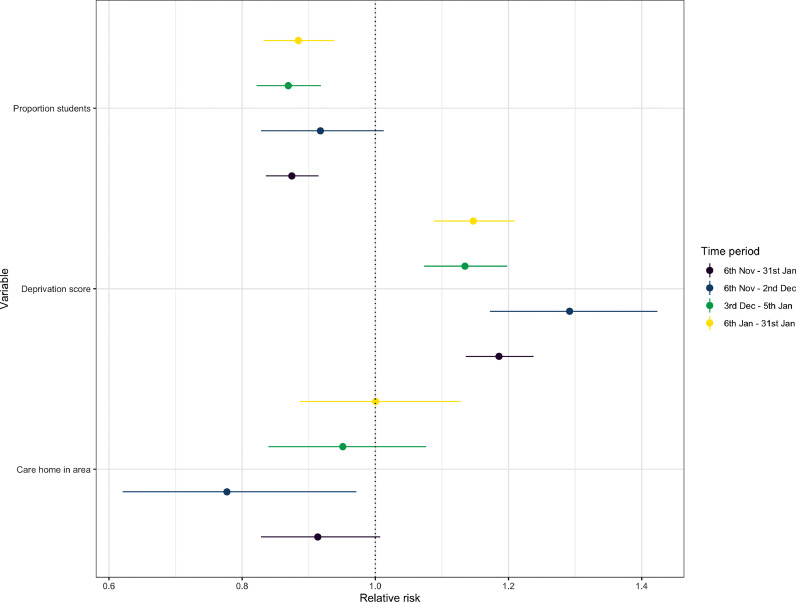
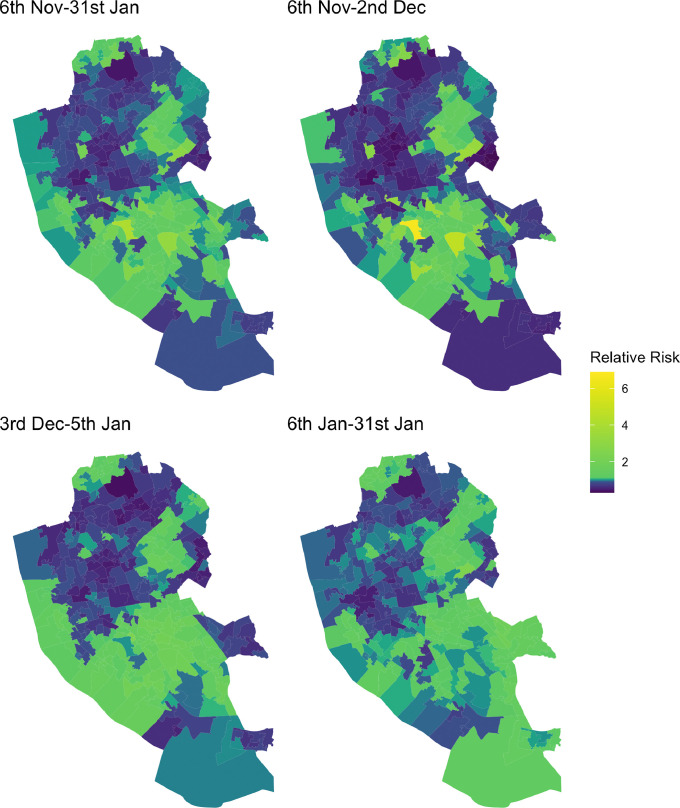
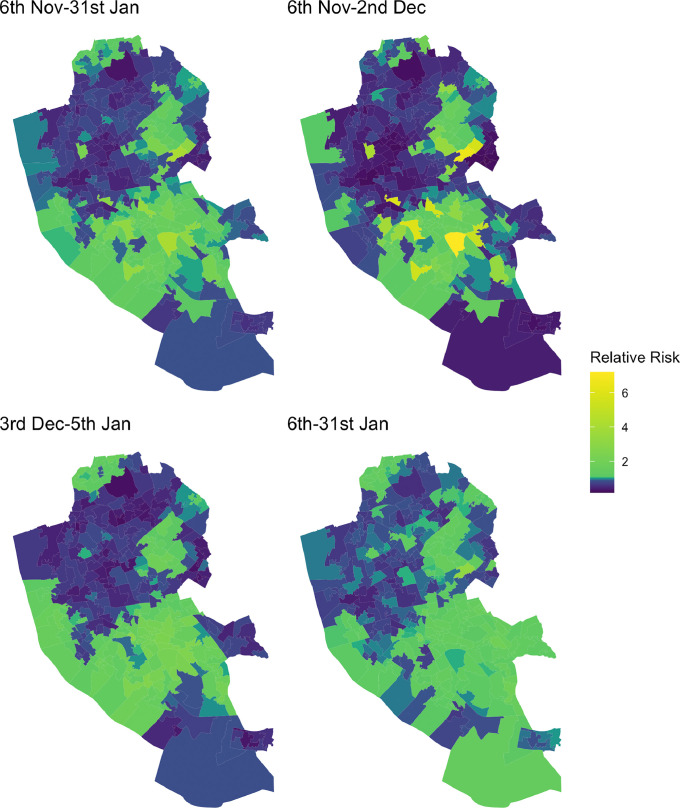
214 525 residents (43%) received a LFT identifying 5192 individuals as positive cases of COVID-19 (1.3% of tests were positive). Uptake was highest in November when there was military assistance. High uptake was observed again in the week preceding Christmas and was sustained into a national lockdown. Overall uptake were lower among males (e.g. 40% uptake over the whole period), Black Asian and other Minority Ethnic groups (e.g. 27% uptake for 'Mixed' ethnicity) and in the most deprived areas (e.g. 32% uptake in most deprived areas). These population groups were also more likely to have received positive tests for COVID-19. Models demonstrated that uptake and repeat testing were lower in areas of higher deprivation, areas located further from test sites and areas containing populations less confident in the using Internet technologies. Positive tests were spatially clustered in deprived areas.
Large-scale voluntary asymptomatic community testing saw social, ethnic, digital and spatial inequalities in uptake. COVID-19 testing and support to isolate need to be more accessible to the vulnerable communities most impacted by the pandemic, including non-digital means of access.
Department of Health and Social Care (UK) and Economic and Social Research Council.
英国利物浦对社区进行大规模新冠病毒无症状检测,作为控制新冠肺炎疫情的一项公共卫生措施。本研究旨在探讨向无新冠肺炎症状人群提供的快速侧向流动新冠病毒抗原检测(LFT)在接受检测及病例检出方面的社会和空间不平等情况。
利用人口健康行动综合情报资源,获取了2020年11月6日至2021年1月31日期间在利物浦接受新冠病毒LFT检测的无症状居民的关联化名记录。采用贝叶斯分层泊松贝萨格、约克和莫利模型来估计检测接受率和阳性率的生态关联。
214525名居民(43%)接受了LFT检测,其中5192人被确定为新冠肺炎阳性病例(检测阳性率为1.3%)。11月在有军事援助时接受率最高。在圣诞节前一周再次观察到高接受率,并持续到全国封锁期间。总体而言,男性(如整个期间接受率为40%)、黑人和少数族裔群体(如“混合”族裔接受率为27%)以及最贫困地区(如最贫困地区接受率为32%)的接受率较低。这些人群也更有可能新冠病毒检测呈阳性。模型表明,在贫困程度较高的地区、距离检测点较远的地区以及对使用互联网技术信心较低的人群所在地区,接受检测和重复检测的比例较低。阳性检测结果在贫困地区呈空间聚集。
大规模自愿无症状社区检测在接受检测方面存在社会、种族、数字和空间不平等。对于受疫情影响最严重的弱势群体,包括非数字获取方式,新冠肺炎检测及隔离支持需要更容易获得。
英国卫生和社会保健部以及经济和社会研究委员会。