Chu Xiang-Peng, Chen Zi-Hao, Lin Shao-Min, Zhang Jia-Tao, Qiu Zhao-Wen, Tang Wen-Fang, Fu Rui, Qiu Zhen-Bin, Yang Xue-Ning, Wu Yi-Long, Nie Qiang, Zhong Wen-Zhao
School of Medicine, South China University of Technology, Guangzhou, China.
Guangdong Lung Cancer Institute, Guangdong Provincial Key Laboratory of Translational Medicine in Lung Cancer, Guangdong Provincial People's Hospital & Guangdong Academy of Medical Sciences, Guangzhou, China.
Transl Lung Cancer Res. 2021 Apr;10(4):1711-1719. doi: 10.21037/tlcr-20-1281.
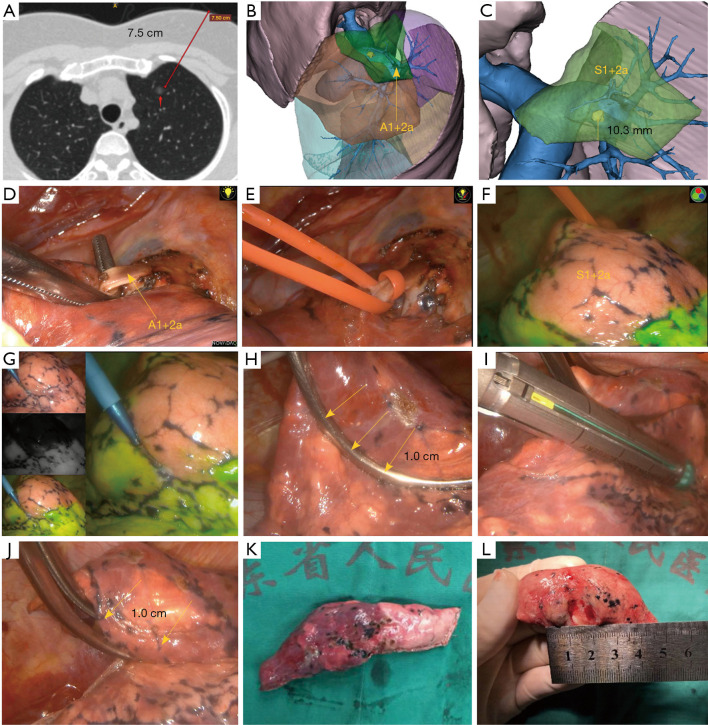
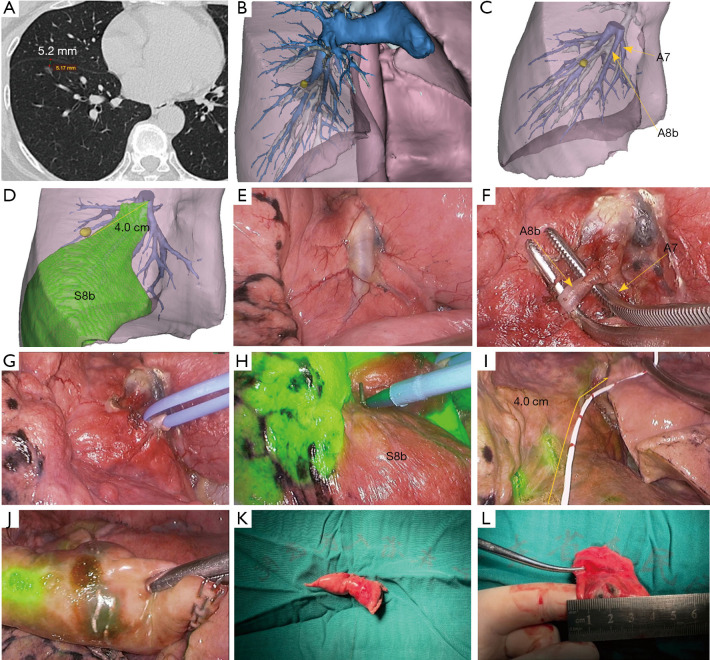
Some pulmonary nodules are not suitable for computed tomography-guided percutaneous localization. This study aimed to investigate the feasibility and safety of real-time localization for these non-palpable pulmonary nodules using watershed analysis of the target pulmonary artery during thoracoscopic wedge resection.
Watershed analysis is a novel technique that can be used to create a specific area on the lung surface for nodule localization. This analysis is performed by temporarily blocking the target pulmonary artery and using indocyanine green fluorescence during surgery. In our study, the surgery was simulated and evaluated preoperatively using a high-precision three-dimensional reconstruction model obtained by multidetector spiral computed tomography. The lung was observed using an infrared thoracoscopy system after an intravenous injection of indocyanine green (2.5 mg/mL), and the white-to-blue transitional zone was marked using electrocautery, after which a wedge resection was performed.
A total of 25 out of 26 patients underwent successful wedge resection. The mean tumor size and depth based on computed tomography scans were 13.2±6.4 and 12.2±7.8 mm, respectively. The mean operation duration was 142.6±52.8 min. The mean bleeding volume during surgery was 12.9±9.7 mL. The mean drainage tube indwelling time was 35.6±20.0 h, and the median length of postoperative stay was 3 days (range, 2-6 days).
Our experience showed that the watershed analysis of the target pulmonary artery for nodule localization was safe and feasible. It may become an effective and attractive alternative method for localizing non-palpable pulmonary nodules in selected patients undergoing thoracoscopic wedge resection.
一些肺结节不适合计算机断层扫描引导下的经皮定位。本研究旨在探讨在胸腔镜楔形切除术中使用目标肺动脉分水岭分析对这些不可触及的肺结节进行实时定位的可行性和安全性。
分水岭分析是一种可用于在肺表面创建特定区域以进行结节定位的新技术。该分析通过在手术期间临时阻断目标肺动脉并使用吲哚菁绿荧光来进行。在我们的研究中,术前使用多排螺旋计算机断层扫描获得的高精度三维重建模型对手术进行模拟和评估。静脉注射吲哚菁绿(2.5mg/mL)后,使用红外胸腔镜系统观察肺,用电灼标记白到蓝的过渡区,然后进行楔形切除。
26例患者中有25例成功进行了楔形切除。基于计算机断层扫描的平均肿瘤大小和深度分别为13.2±6.4和12.2±7.8mm。平均手术时间为142.6±52.8分钟。手术期间的平均出血量为12.9±9.7mL。引流管平均留置时间为35.6±20.0小时,术后中位住院时间为3天(范围2 - 6天)。
我们的经验表明,对目标肺动脉进行分水岭分析以定位结节是安全可行的。它可能成为在接受胸腔镜楔形切除术的选定患者中定位不可触及肺结节的一种有效且有吸引力的替代方法。