Department of Cardiovascular Sciences and the NIHR Leicester Biomedical Research Centre, Glenfield Hospital, University of Leicester; University Hospitals of Leicester NHS Trust, Leicester, United Kingdom.
Institute of Cardiovascular Sciences, University of Birmingham, Birmingham, United Kingdom.
J Am Coll Cardiol. 2021 May 25;77(20):2466-2476. doi: 10.1016/j.jacc.2021.03.309.
Published data suggest worse outcomes in acute coronary syndrome (ACS) patients and concurrent coronavirus disease 2019 (COVID-19) infection. Mechanisms remain unclear.
The purpose of this study was to report the demographics, angiographic findings, and in-hospital outcomes of COVID-19 ACS patients and compare these with pre-COVID-19 cohorts.
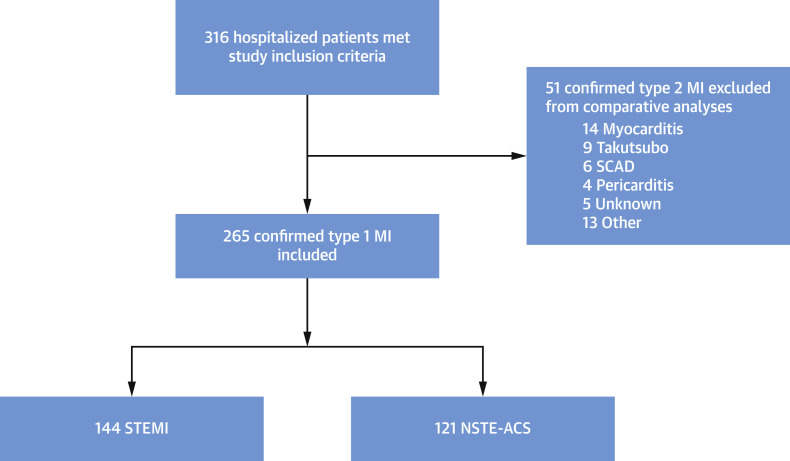
From March 1, 2020 to July 31, 2020, data from 55 international centers were entered into a prospective, COVID-ACS Registry. Patients were COVID-19 positive (or had a high index of clinical suspicion) and underwent invasive coronary angiography for suspected ACS. Outcomes were in-hospital major cardiovascular events (all-cause mortality, re-myocardial infarction, heart failure, stroke, unplanned revascularization, or stent thrombosis). Results were compared with national pre-COVID-19 databases (MINAP [Myocardial Ischaemia National Audit Project] 2019 and BCIS [British Cardiovascular Intervention Society] 2018 to 2019).
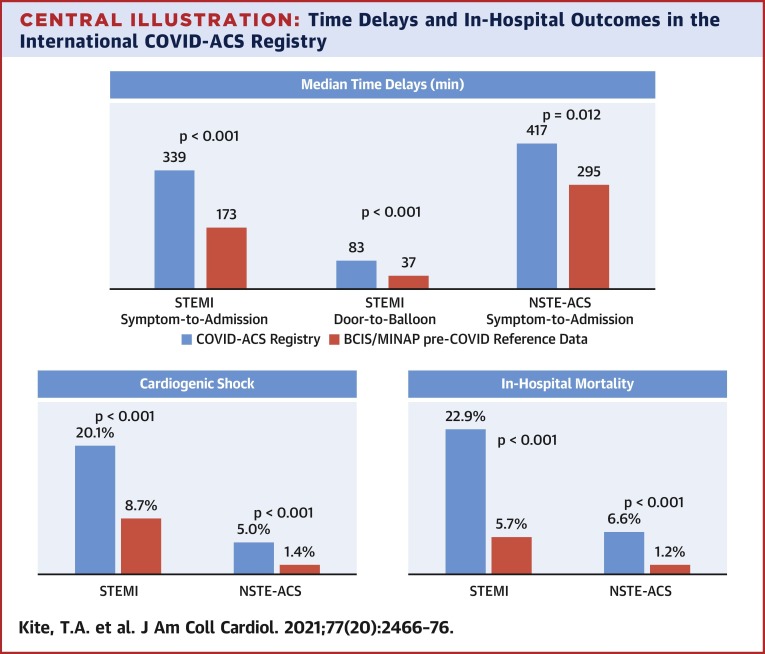
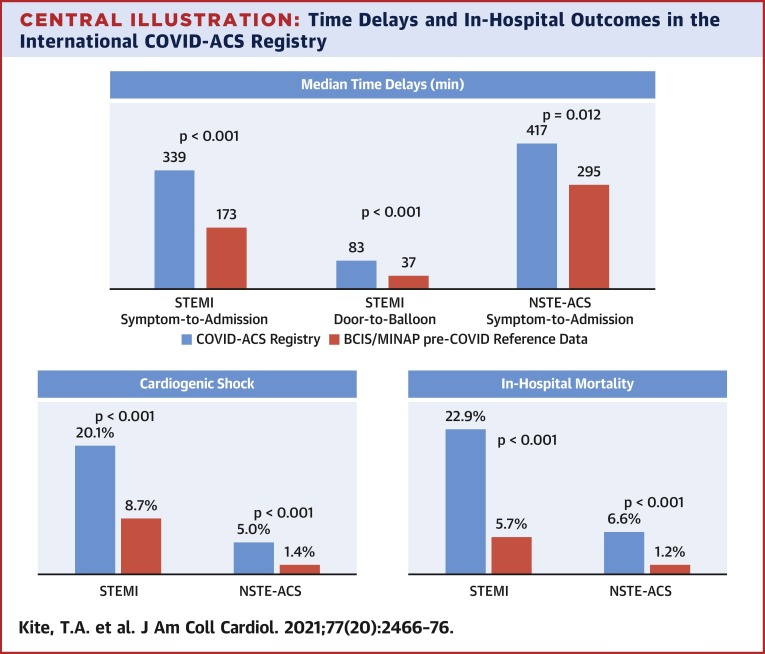
In 144 ST-segment elevation myocardial infarction (STEMI) and 121 non-ST-segment elevation acute coronary syndrome (NSTE-ACS) patients, symptom-to-admission times were significantly prolonged (COVID-STEMI vs. BCIS: median 339.0 min vs. 173.0 min; p < 0.001; COVID NSTE-ACS vs. MINAP: 417.0 min vs. 295.0 min; p = 0.012). Mortality in COVID-ACS patients was significantly higher than BCIS/MINAP control subjects in both subgroups (COVID-STEMI: 22.9% vs. 5.7%; p < 0.001; COVID NSTE-ACS: 6.6% vs. 1.2%; p < 0.001), which remained following multivariate propensity analysis adjusting for comorbidities (STEMI subgroup odds ratio: 3.33 [95% confidence interval: 2.04 to 5.42]). Cardiogenic shock occurred in 20.1% of COVID-STEMI patients versus 8.7% of BCIS patients (p < 0.001).
In this multicenter international registry, COVID-19-positive ACS patients presented later and had increased in-hospital mortality compared with a pre-COVID-19 ACS population. Excessive rates of and mortality from cardiogenic shock were major contributors to the worse outcomes in COVID-19 positive STEMI patients.
已有研究表明,合并 2019 年冠状病毒病(COVID-19)的急性冠状动脉综合征(ACS)患者预后更差。但其具体机制仍不明确。
本研究旨在报告 COVID-19 合并 ACS 患者的人口统计学、血管造影结果和院内结局,并与 COVID-19 前队列进行比较。
2020 年 3 月 1 日至 2020 年 7 月 31 日,55 个国际中心的数据被纳入前瞻性 COVID-ACS 登记处。患者 COVID-19 检测阳性(或具有高度临床疑似),并因疑似 ACS 而行有创冠状动脉造影。主要院内心血管事件(全因死亡率、再心肌梗死、心力衰竭、卒中和计划外血运重建或支架血栓形成)为观察终点。结果与国家 COVID-19 前数据库(MINAP [心肌缺血国家审计项目] 2019 年和 BCIS [英国心血管介入学会] 2018 年至 2019 年)进行了比较。
在 144 例 ST 段抬高型心肌梗死(STEMI)和 121 例非 ST 段抬高型急性冠状动脉综合征(NSTE-ACS)患者中,症状出现至入院的时间明显延长(COVID-STEMI 与 BCIS:中位时间 339.0 分钟比 173.0 分钟;p<0.001;COVID NSTE-ACS 与 MINAP:中位时间 417.0 分钟比 295.0 分钟;p=0.012)。COVID-ACS 患者的死亡率明显高于 BCIS/MINAP 对照组,且在两个亚组中均具有统计学意义(COVID-STEMI:22.9%比 5.7%;p<0.001;COVID NSTE-ACS:6.6%比 1.2%;p<0.001),在对共病进行多变量倾向评分分析后仍具有统计学意义(STEMI 亚组比值比:3.33 [95%置信区间:2.04 至 5.42])。COVID-STEMI 患者中有 20.1%发生心原性休克,而 BCIS 患者中仅为 8.7%(p<0.001)。
在这项多中心国际登记研究中,COVID-19 阳性 ACS 患者较 COVID-19 前 ACS 患者就诊时间更晚,院内死亡率更高。心原性休克的发生率和死亡率过高是 COVID-19 阳性 STEMI 患者预后更差的主要原因。