Nephrology Division, Federal University of São Paulo, São Paulo, Brazil.
Laboratory of Applied Computing (LABCOM), Federal Institute of Education, Science and Technology of São Paulo, São Paulo, Brazil.
PLoS One. 2021 May 25;16(5):e0251048. doi: 10.1371/journal.pone.0251048. eCollection 2021.
COVID-19 is a multisystemic disorder that frequently causes acute kidney injury (AKI). However, the precise clinical and biochemical variables associated with AKI progression in patients with severe COVID-19 remain unclear.
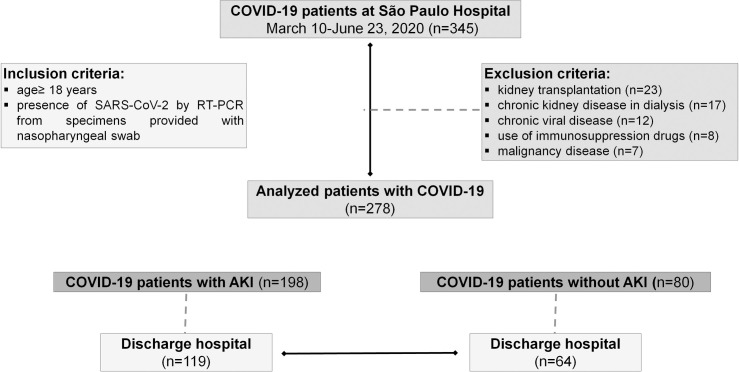
We performed a retrospective study on 278 hospitalized patients who were admitted to the ward and intensive care unit (ICU) with COVID-19 between March 2020 and June 2020, at the University Hospital, São Paulo, Brazil. Patients aged ≥ 18 years with COVID-19 confirmed on RT-PCR were included. AKI was defined according to the Kidney Disease Improving Global Outcomes (KDIGO) criteria. We evaluated the incidence of AKI, several clinical variables, medicines used, and outcomes in two sub-groups: COVID-19 patients with AKI (Cov-AKI), and COVID-19 patients without AKI (non-AKI). Univariate and multivariate analyses were performed.
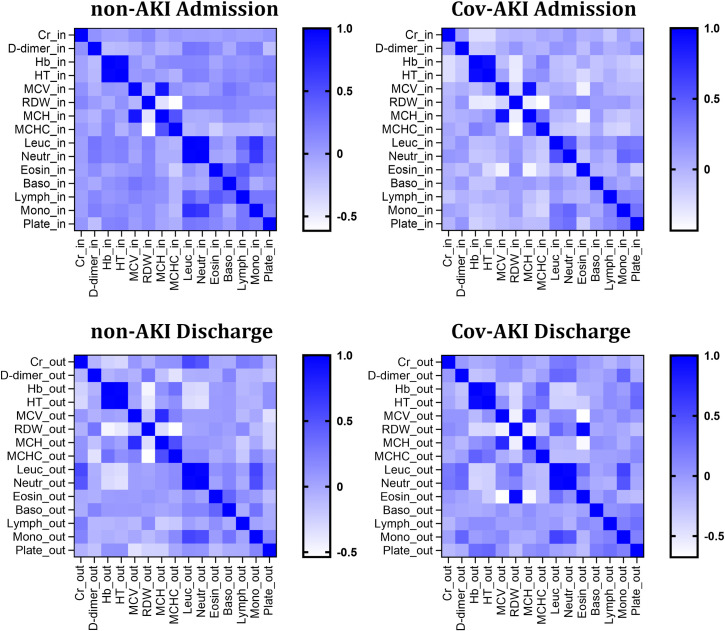
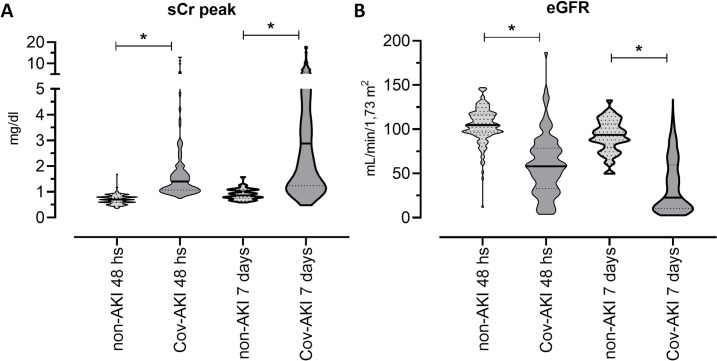
First, an elevated incidence of AKI (71.2%) was identified, distributed across different stages of the KDIGO criteria. We further observed higher levels of creatinine, C-reactive protein (CRP), leukocytes, neutrophils, monocytes, and neutrophil-to-lymphocyte ratio (NLR) in the Cov-AKI group than in the non-AKI group, at hospital admission. On univariate analysis, Cov-AKI was associated with older age (>62 years), hypertension, CRP, MCV, leucocytes, neutrophils, NLR, combined hydroxychloroquine and azithromycin treatment, use of mechanical ventilation, and vasoactive drugs. Multivariate analysis showed that hypertension and the use of vasoactive drugs were independently associated with a risk of higher AKI in COVID-19 patients. Finally, we preferentially found an altered erythrocyte and leukocyte cellular profile in the Cov-AKI group compared to the non-AKI group, at hospital discharge.
In our study, the development of AKI in patients with severe COVID-19 was related to inflammatory blood markers and therapy with hydroxychloroquine/azithromycin, with vasopressor requirement and hypertension considered potential risk factors. Thus, attention to the protocol, hypertension, and some blood markers may help assist doctors with decision-making for the management of COVID-19 patients with AKI.
COVID-19 是一种多系统疾病,常导致急性肾损伤(AKI)。然而,严重 COVID-19 患者 AKI 进展相关的确切临床和生化变量仍不清楚。
我们对 2020 年 3 月至 6 月期间在巴西圣保罗大学医院因 COVID-19 住院和入住重症监护病房(ICU)的 278 名住院患者进行了回顾性研究。纳入年龄≥18 岁、经 RT-PCR 确诊 COVID-19 的患者。AKI 根据肾脏病改善全球结局(KDIGO)标准定义。我们评估了 AKI 的发生率、几个临床变量、使用的药物以及 COVID-19 伴有 AKI(Cov-AKI)和 COVID-19 不伴有 AKI(非 AKI)两组患者的结局。进行了单变量和多变量分析。
首先,我们发现 AKI 的发生率很高(71.2%),分布在 KDIGO 标准的不同阶段。我们还观察到 Cov-AKI 组入院时肌酐、C 反应蛋白(CRP)、白细胞、中性粒细胞、单核细胞和中性粒细胞与淋巴细胞比值(NLR)水平高于非 AKI 组。单变量分析显示,Cov-AKI 与年龄较大(>62 岁)、高血压、CRP、MCV、白细胞、中性粒细胞、NLR、联合羟氯喹和阿奇霉素治疗、使用机械通气和血管活性药物有关。多变量分析显示,高血压和血管活性药物的使用与 COVID-19 患者 AKI 风险增加独立相关。最后,与非 AKI 组相比,我们在 Cov-AKI 组患者出院时更优先发现红细胞和白细胞细胞谱改变。
在我们的研究中,严重 COVID-19 患者 AKI 的发展与炎症血液标志物以及羟氯喹/阿奇霉素治疗有关,血管加压素需求和高血压被认为是潜在的危险因素。因此,关注方案、高血压和一些血液标志物可能有助于协助医生为 AKI 患者的 COVID-19 管理做出决策。