Department of Internal Medicine, Clinica Nefrologica Dialisi e Trapianto, University of Genoa, Hospital Policlinico San Martino, IRCCS, Viale Benedetto XV, 16132, Genoa, Italy.
Department of Health Sciences, Infectious Diseases Clinic, University of Genoa, Hospital Policlinico San Martino-IRCCS, Genoa, Italy.
J Nephrol. 2021 Feb;34(1):173-183. doi: 10.1007/s40620-020-00875-1. Epub 2020 Oct 6.
The prevalence of kidney involvement during SARS-CoV-2 infection has been reported to be high. Nevertheless, data are lacking about the determinants of acute kidney injury (AKI) and the combined effect of chronic kidney disease (CKD) and AKI in COVID-19 patients.
We collected data on patient demographics, comorbidities, chronic medications, vital signs, baseline laboratory test results and in-hospital treatment in patients with COVID-19 consecutively admitted to our Institution. Chronic kidney disease was defined as eGFR < 60 mL/min per 1.73 m or proteinuria at urinalysis within 180 days prior to hospital admission. AKI was defined according to KDIGO criteria. The primary and secondary outcomes were the development of AKI and death.
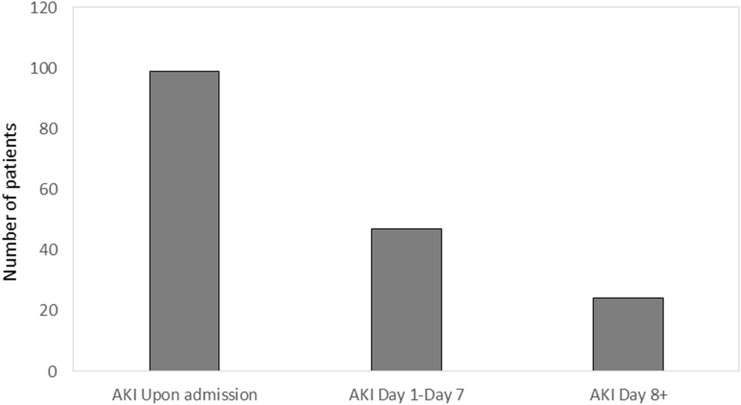
Of 777 patients eligible for the study, acute kidney injury developed in 176 (22.6%). Of these, 79 (45%) showed an acute worsening of a preexisting CKD, and 21 (12%) required kidney replacement therapy. Independent associates of AKI were chronic kidney disease, C-reactive protein (CRP) and ventilation support. Among patients with acute kidney injury, 111 died (63%) and its occurrence increased the risk of death by 60% (HR 1.60 [95% IC 1.21-2.49] p = 0.002) independently of potential confounding factors including hypertension, preexisting kidney damage, and comorbidities. Patients with AKI showed a significantly higher rate of deaths attributed to bleeding compared to CKD and the whole population (7.5 vs 1.5 vs 3.5%, respectively).
Awareness of kidney function, both preexisting CKD and development of acute kidney injury, may help to identify those patients at increased risk of death.
已有报道称,在 SARS-CoV-2 感染期间,肾脏受累的患病率很高。然而,关于急性肾损伤(AKI)的决定因素以及 COVID-19 患者中慢性肾脏病(CKD)和 AKI 的联合影响的数据仍很缺乏。
我们连续收集了我院收治的 COVID-19 患者的人口统计学、合并症、慢性药物治疗、生命体征、基线实验室检查结果和住院治疗数据。慢性肾脏病定义为入院前 180 天内 eGFR<60 mL/min/1.73 m 或尿液分析中有蛋白尿。AKI 根据 KDIGO 标准定义。主要和次要结局为 AKI 发展和死亡。
在符合研究条件的 777 名患者中,176 名(22.6%)发生 AKI。其中,79 名(45%)表现为预先存在的 CKD 的急性恶化,21 名(12%)需要肾脏替代治疗。AKI 的独立相关因素包括慢性肾脏病、C 反应蛋白(CRP)和通气支持。在发生 AKI 的患者中,111 名(63%)死亡,其发生使死亡风险增加了 60%(HR 1.60[95%CI 1.21-2.49],p=0.002),独立于潜在的混杂因素,包括高血压、预先存在的肾脏损伤和合并症。与 CKD 和整个人群相比,发生 AKI 的患者因出血导致的死亡率明显更高(分别为 7.5%、1.5%和 3.5%)。
了解肾功能,包括预先存在的 CKD 和 AKI 的发展,可能有助于识别那些死亡风险增加的患者。