Usui Takami, Suzuki Kazufumi, Niinami Hiroshi, Sakai Shuji
Department of Diagnostic Imaging and Nuclear Medicine, Tokyo Women's Medical University, 8-1, Kawada-cho, Shinjuku-ku, Tokyo, 162-8666, Japan.
Department of Cardiovascular Surgery, Tokyo Women's Medical University, 8-1, Kawada-cho, Shinjuku-ku, Tokyo, 162-8666, Japan.
J Med Case Rep. 2021 May 26;15(1):299. doi: 10.1186/s13256-021-02850-1.
Aortic dissection is one of the causes of stroke. Because cerebral infarction with aortic dissection is a contraindication to intravenous recombinant tissue plasminogen activator (rt-PA) therapy, exclusion of aortic dissection is necessary prior to its administration. However, imaging takes time to provide a diagnosis, possibly causing delays in surgical treatment.
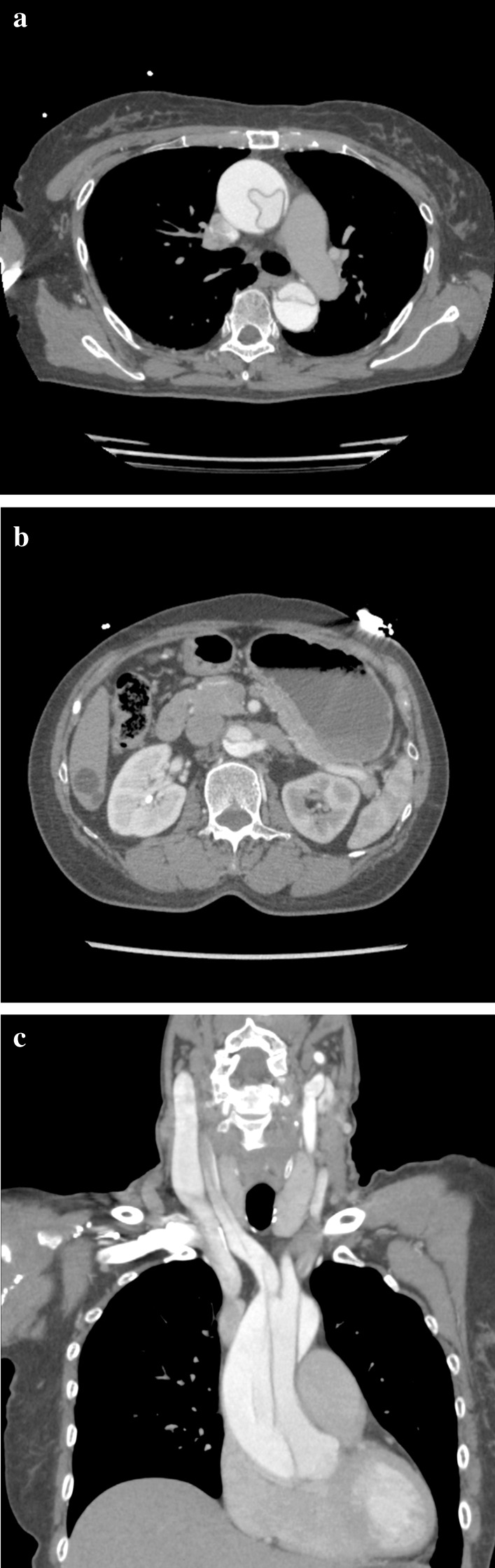
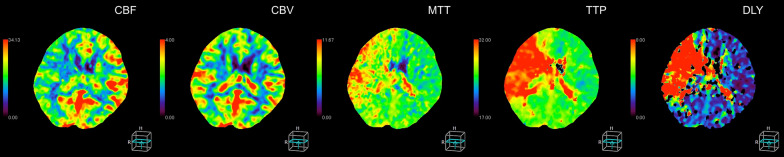
A 65-year-old Japanese female patient was transported to the hospital for a suspected stroke, with back pain and left upper and lower extremity palsy which occurred while eating. Upon arrival at the hospital, the left lower limb paralysis had improved, but the left upper limb paralysis remained. Right back pain had also developed. A plain head computed tomography (CT) scan performed 110 minutes after onset showed no acute bleeding or infarction. Subsequent CT perfusion (CTP) showed acute perfusion disturbance in the right hemisphere without infarction, known as ischemic penumbra. The four-dimensional maximum-intensity projection image reconstructed from CTP showed a delayed enhancement at the right internal carotid and right middle cerebral arteries compared to the contralateral side, suggesting a proximal vascular lesion. Contrast helical CT from the neck to abdomen revealed an acute aortic dissection of Stanford type A with false lumen patency. The dissection extended to the proximal right common carotid artery. The patient underwent an emergency total arch replacement and open stent graft. After recovering well, the patient was ambulatory upon discharge from the hospital. The combination of plain head CT, CTP, and helical CT scan from the neck to abdomen enabled us to evaluate for stroke and aortic dissection within a short amount of time, allowing for early therapeutic intervention.
When acute stroke is suspected due to neurological deficits, plain head CT is the first choice for imaging diagnosis. The addition of cervical CT angiography can reliably exclude stroke due to aortic dissection. CTP can identify ischemic penumbra, which cannot be diagnosed by plain head CT or diffusion-weighted magnetic resonance imaging. These combined stroke CT protocols helped us avoid missing an aortic dissection.
主动脉夹层是卒中的病因之一。由于伴有主动脉夹层的脑梗死是静脉注射重组组织型纤溶酶原激活剂(rt-PA)治疗的禁忌证,因此在给药前必须排除主动脉夹层。然而,影像学检查需要时间来做出诊断,这可能会导致手术治疗延迟。
一名65岁的日本女性患者因疑似卒中被送往医院,患者在进食时出现背痛以及左上肢和下肢麻痹。入院时,左下肢麻痹有所改善,但左上肢麻痹仍然存在。同时还出现了右背痛。发病110分钟后进行的头颅平扫计算机断层扫描(CT)未显示急性出血或梗死。随后的CT灌注(CTP)显示右半球存在急性灌注紊乱但无梗死,即缺血半暗带。从CTP重建的四维最大强度投影图像显示,与对侧相比,右侧颈内动脉和大脑中动脉延迟强化,提示近端血管病变。从颈部到腹部的对比螺旋CT显示为Stanford A型急性主动脉夹层,假腔通畅。夹层延伸至右侧颈总动脉近端。患者接受了急诊全弓置换和开放式支架植入术。恢复良好后,患者出院时可独立行走。头颅平扫CT、CTP以及从颈部到腹部的螺旋CT扫描相结合,使我们能够在短时间内评估卒中及主动脉夹层情况,从而实现早期治疗干预。
当因神经功能缺损怀疑急性卒中时,头颅平扫CT是影像学诊断的首选。增加颈部CT血管造影可以可靠地排除主动脉夹层所致的卒中。CTP可以识别缺血半暗带,这是头颅平扫CT或扩散加权磁共振成像无法诊断的。这些联合的卒中CT方案有助于我们避免漏诊主动脉夹层。