Rugo Hope S, Cristofanilli Massimo, Loibl Sybille, Harbeck Nadia, DeMichele Angela, Iwata Hiroji, Park Yoon Hee, Brufsky Adam, Theall Kathy Puyana, Huang Xin, McRoy Lynn, Bananis Eustratios, Turner Nicholas C
Department of Medicine (Hematology/Oncology), University of California San Francisco, Helen Diller Family Comprehensive Cancer Center, San Francisco, California, USA.
Division of Hematology/Oncology, Robert H. Lurie Comprehensive Cancer Center, Feinberg School of Medicine, Chicago, Illinois, USA.
Oncologist. 2021 Aug;26(8):e1339-e1346. doi: 10.1002/onco.13833. Epub 2021 Jun 12.
This analysis investigated whether baseline characteristics affect the survival benefit derived from palbociclib-fulvestrant and the optimal timing of cyclin-dependent kinase 4/6 inhibitor therapy for advanced breast cancer (ABC) in patients from PALOMA-3.
In total, 521 patients were randomized 2:1 to receive palbociclib (125 mg/day, 3/1 schedule)-fulvestrant (500 mg, intramuscular injection, on days 1 and 15 of cycle 1, and then day 1 of each subsequent cycle) or matching placebo-fulvestrant. Median overall survival (OS) and progression-free survival were estimated using the Kaplan-Meier method.
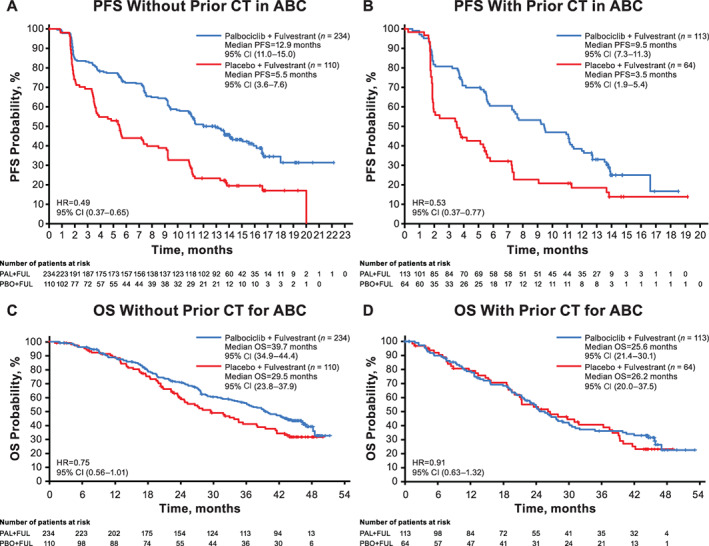
Multivariable analysis identified endocrine sensitivity, nonvisceral disease, no prior chemotherapy for ABC, and Eastern Cooperative Oncology Group performance status (ECOG PS) of 0 as significant prognostic factors for OS. Patients without chemotherapy for ABC had fewer prior lines of treatment in any setting and in the ABC setting versus patients with prior chemotherapy for ABC (two or fewer prior systemic therapies: 69% vs. 42%; no more than one prior line for ABC: 82% vs. 33%, respectively). Median OS was prolonged with palbociclib-fulvestrant in patients without prior chemotherapy for ABC (39.7 vs. 29.5 months; hazard ratio, 0.75; 95% confidence interval [CI]: 0.56-1.01) and was similar in patients with prior chemotherapy for ABC (25.6 vs. 26.2 months; hazard ratio, 0.91 [95% CI: 0.63-1.32]) versus placebo-fulvestrant.
Prognostic factors for OS included endocrine sensitivity, nonvisceral disease, ECOG PS of 0, and no prior chemotherapy for ABC. Exploratory analyses suggest improved OS with palbociclib-fulvestrant versus placebo-fulvestrant in patients with no prior chemotherapy for ABC, prior endocrine sensitivity, and fewer prior regimens of systemic therapy. (Clinical trial identification number: NCT01942135).
Prognostic factors for overall survival in HR+/HER2- advanced breast cancer (ABC) include the absence of prior chemotherapy in the advanced setting, endocrine sensitivity, nonvisceral disease, and an ECOG performance status of 0. Improved overall survival benefit was observed with palbociclib-fulvestrant versus placebo-fulvestrant in patients (regardless of menopausal status or visceral involvement) with no prior chemotherapy for ABC, with prior endocrine sensitivity, and fewer prior regimens of systemic therapy. Progression-free survival was prolonged with palbociclib across subgroups (regardless of chemotherapy exposure in ABC). These exploratory findings suggest that patients may receive greater clinical benefit from palbociclib-fulvestrant if they receive the combination before chemotherapy in the advanced setting.
本分析探讨了基线特征是否会影响从哌柏西利-氟维司群中获得的生存获益,以及在PALOMA-3研究的晚期乳腺癌(ABC)患者中细胞周期蛋白依赖性激酶4/6抑制剂治疗的最佳时机。
总共521例患者按2:1随机分组,接受哌柏西利(125mg/天,3/1给药方案)-氟维司群(500mg,肌肉注射,第1周期第1天和第15天,随后每个周期第1天)或匹配的安慰剂-氟维司群。采用Kaplan-Meier方法估计中位总生存期(OS)和无进展生存期。
多变量分析确定内分泌敏感性、非内脏疾病、未接受过ABC的化疗以及东部肿瘤协作组体能状态(ECOG PS)为0是OS的重要预后因素。与接受过ABC化疗的患者相比,未接受过ABC化疗的患者在任何情况下以及在ABC情况下的既往治疗线数更少(既往全身治疗2线或更少:69%对42%;ABC既往治疗线数不超过1线:分别为82%对33%)。在未接受过ABC化疗的患者中,哌柏西利-氟维司群可延长中位OS(39.7个月对二十九点五个月;风险比,0.75;95%置信区间[CI]:0.56-1.01),在接受过ABC化疗的患者中与安慰剂-氟维司群相似(二十五点六个月对二十六点二个月;风险比,0.91[95%CI:0.63-1.32])。
OS的预后因素包括内分泌敏感性、非内脏疾病、ECOG PS为0以及未接受过ABC的化疗。探索性分析表明,在未接受过ABC化疗、既往内分泌敏感且既往全身治疗方案较少的患者中,与安慰剂-氟维司群相比,哌柏西利-氟维司群可改善OS。(临床试验识别号:NCT01942135)
HR+/HER2-晚期乳腺癌(ABC)总生存期的预后因素包括晚期未接受过化疗、内分泌敏感性、非内脏疾病以及ECOG体能状态为0。在未接受过ABC化疗、既往内分泌敏感且既往全身治疗方案较少的患者(无论绝经状态或内脏受累情况)中,与安慰剂-氟维司群相比,哌柏西利-氟维司群可改善总生存获益。在各亚组中(无论ABC中是否接受过化疗),哌柏西利均可延长无进展生存期。这些探索性发现表明,如果患者在晚期化疗前接受联合治疗,可能从哌柏西利-氟维司群中获得更大的临床获益。