Department of Thoracic and Cardiovascular Surgery, Bucheon St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea.
Department of Thoracic and Cardiovascular Surgery, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea.
Thorac Cancer. 2021 Jul;12(13):1952-1958. doi: 10.1111/1759-7714.13984. Epub 2021 May 25.
Patients with early lung cancer are the best candidates for surgical resection. However, those patients with high grade patterns (micropapillary or solid) do not have a good prognosis, even if they have been diagnosed with stage I lung adenocarcinoma. A new modified grading system has been introduced and this study aimed to identify the prognostic role of the new grading system in patients with stage IA lung adenocarcinoma.
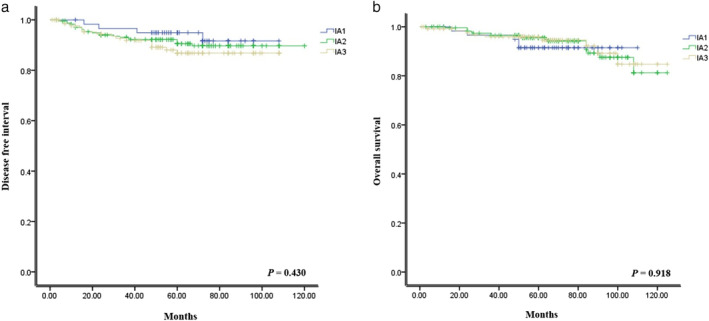
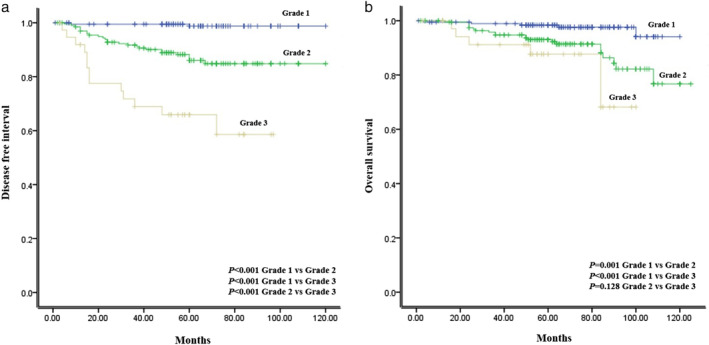
Patients with pathological stage IA lung adenocarcinoma, according to the eighth TNM classification who underwent curative resection, were reviewed. The pathological data of stage IA adenocarcinoma was reviewed 1 (grade 1: lepidic predominant with no or less than 20% of high grade patterns, grade 2: acinar or papillary predominant with no or less than 20% of high grade patterns, grade 3: any tumor with 20% or more of high grade patterns). Prognostic factors were analyzed for disease-free interval (DFI) and overall survival (OS) using Cox proportional models.
The medical records of 429 patients with stage IA lung adenocarcinoma were reviewed. DFI (p < 0.001) and OS (p < 0.001) were significantly lower in patients diagnosed with grade 3 compared with grade 1 and grade 2. Multivariate analysis showed that smoking (p = 0.013), value of SUVmax (p = 0.005), lymphovascular invasion (p = 0.004) and grade 3 (p = 0.008) were significant prognostic factors for DFI.
The proportion of high grade patterns showed a different prognosis, even if curative resection had been performed for stage IA adenocarcinoma. This new grading system is more simple and useful in the prediction of a prognosis in patients with stage IA lung adenocarcinoma.
早期肺癌患者是手术切除的最佳人选。然而,那些具有高级别模式(微乳头状或实体状)的患者预后不佳,即使他们被诊断为 I 期肺腺癌。已经引入了一种新的改良分级系统,本研究旨在确定新分级系统在 I 期肺腺癌患者中的预后作用。
回顾了根据第八版 TNM 分类接受根治性切除的病理分期为 IA 期肺腺癌患者。回顾了 IA 期腺癌的病理数据,分为 1 级(贴壁为主,高级别模式比例小于等于 20%)、2 级(腺泡或乳头为主,高级别模式比例小于等于 20%)、3 级(任何肿瘤高级别模式比例大于 20%)。使用 Cox 比例模型分析无病间隔(DFI)和总生存(OS)的预后因素。
回顾了 429 例 IA 期肺腺癌患者的病历。DFI(p<0.001)和 OS(p<0.001)在 3 级患者中明显低于 1 级和 2 级患者。多变量分析显示,吸烟(p=0.013)、SUVmax 值(p=0.005)、血管淋巴管侵犯(p=0.004)和 3 级(p=0.008)是 DFI 的显著预后因素。
即使对 IA 期腺癌进行了根治性切除,高级别模式的比例也显示出不同的预后。这种新的分级系统在预测 IA 期肺腺癌患者的预后方面更加简单和有效。