Department of Physiology and Cell Biology, University of Nevada School of Medicine, Reno, NV 89557, United States.
Department of Medicine, Renown Health, Reno, NV 89557, United States.
World J Gastroenterol. 2021 May 21;27(19):2341-2352. doi: 10.3748/wjg.v27.i19.2341.
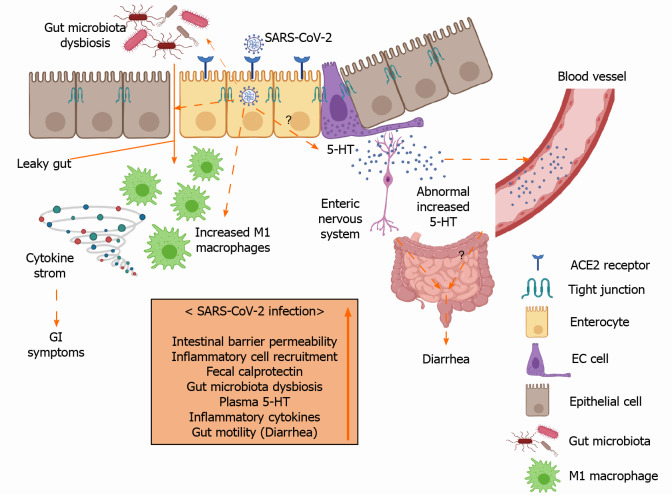
Gastrointestinal (GI) symptoms, such as diarrhea, abdominal pain, vomiting, and anorexia, are frequently observed in patients with coronavirus disease 2019 (COVID-19). However, the pathophysiological mechanisms connecting these GI symptoms to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infections remain elusive. Previous studies indicate that the entry of SARS-CoV-2 into intestinal cells leads to downregulation of angiotensin converting enzyme 2 (ACE2) receptors resulting in impaired barrier function. While intestinal ACE2 functions as a chaperone for the amino acid transporter B0AT1, the B0AT1/ACE2 complex within the intestinal epithelium acts as a regulator of gut microbiota composition and function. Alternations to the B0AT1/ACE2 complex lead to microbial dysbiosis through increased local and systemic immune responses. Previous studies have also suggested that altered serotonin metabolism may be the underlying cause of GI disorders involving diarrhea. The findings of elevated plasma serotonin levels and high fecal calprotectin in COVID-19 patients with diarrhea indicate that the viral infection evokes a systemic inflammatory response that specifically involves the GI. Interestingly, the elevated proinflammatory cytokines correlate with elevated serotonin and fecal calprotectin levels further supporting the evidence of GI inflammation, a hallmark of functional GI disorders. Moreover, the finding that rectal swabs of COVID-19 patients remain positive for SARS-CoV-2 even after the nasopharynx clears the virus, suggests that viral replication and shedding from the GI tract may be more robust than that of the respiratory tract, further indicating fecal-oral transmission as another important route of viral spread. This review summarized the evidence for pathophysiological mechanisms (impaired barrier function, gut inflammation, altered serotonin metabolism and gut microbiota dysbiosis) underlying the GI symptoms in patients with COVID-19.
胃肠道(GI)症状,如腹泻、腹痛、呕吐和食欲不振,在 COVID-19 患者中经常观察到。然而,将这些胃肠道症状与严重急性呼吸综合征冠状病毒 2(SARS-CoV-2)感染联系起来的病理生理机制仍不清楚。先前的研究表明,SARS-CoV-2 进入肠道细胞会导致血管紧张素转换酶 2(ACE2)受体下调,从而导致屏障功能受损。虽然肠道 ACE2 作为氨基酸转运体 B0AT1 的伴侣,但肠道上皮细胞中的 B0AT1/ACE2 复合物作为肠道微生物群落组成和功能的调节剂。B0AT1/ACE2 复合物的改变会通过增加局部和全身免疫反应导致微生物失调。先前的研究还表明,改变的 5-羟色胺代谢可能是涉及腹泻的胃肠道疾病的根本原因。COVID-19 腹泻患者血浆 5-羟色胺水平升高和粪便钙卫蛋白升高的发现表明,病毒感染引发了一种特定涉及胃肠道的全身性炎症反应。有趣的是,升高的促炎细胞因子与升高的 5-羟色胺和粪便钙卫蛋白水平相关,进一步支持了胃肠道炎症的证据,这是功能性胃肠道疾病的标志。此外,发现 COVID-19 患者的直肠拭子即使在鼻咽清除病毒后仍能检测到 SARS-CoV-2 阳性,这表明病毒从胃肠道的复制和脱落可能比呼吸道更强烈,这进一步表明粪便-口腔传播是另一种重要的病毒传播途径。这篇综述总结了 COVID-19 患者胃肠道症状的病理生理机制(屏障功能受损、肠道炎症、5-羟色胺代谢改变和肠道微生物失调)的证据。