Internal Medicine Department, IMIBIC/Reina Sofia University Hospital/University of Córdoba, Avda. Menéndez Pidal s/n, 14004 Córdoba, Spain.
CIBER Fisiopatologia Obesidad y Nutrición (CIBEROBN), Instituto de Salud Carlos III, 28029 Madrid, Spain.
Nutrients. 2021 May 21;13(6):1760. doi: 10.3390/nu13061760.
Calcifediol has been proposed as a potential treatment for COVID-19 patients.
To compare the administration or not of oral calcifediol on mortality risk of patients hospitalized because of COVID-19.
Retrospective, multicenter, open, non-randomized cohort study.
Hospitalized care.
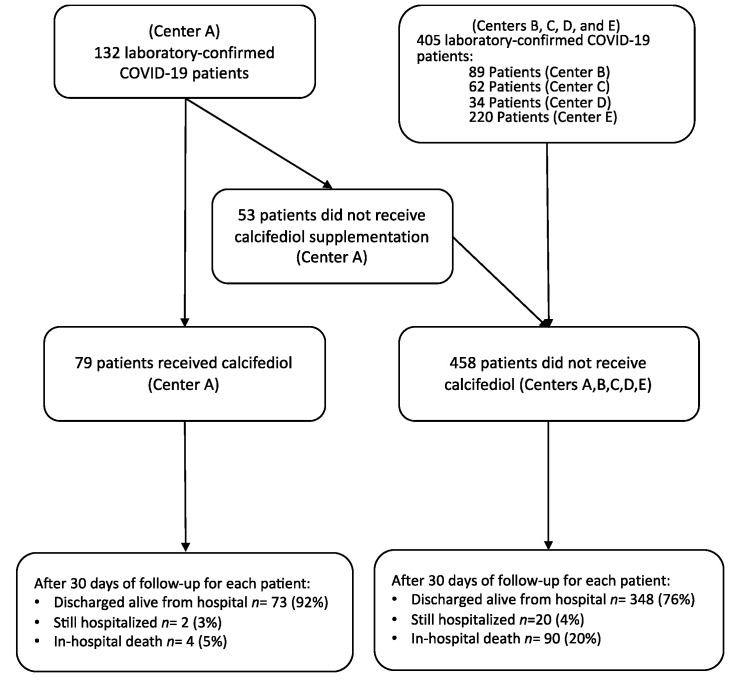
Patients with laboratory-confirmed COVID-19 between 5 February and 5 May 2020 in five hospitals in the South of Spain.
Patients received calcifediol (25-hydroxyvitamin D) treatment (0.266 mg/capsule, 2 capsules on entry and then one capsule on day 3, 7, 14, 21, and 28) or not.
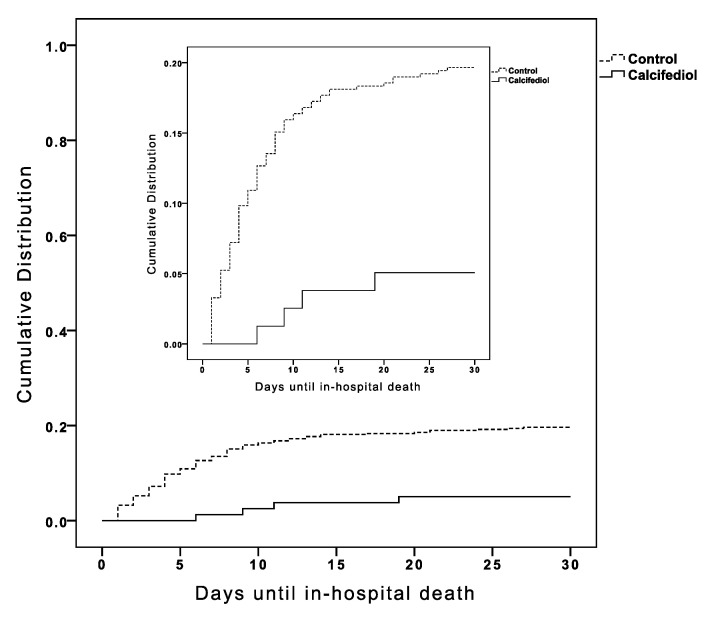
In-hospital mortality during the first 30 days after admission.
A total of 537 patients were hospitalized with COVID-19 (317 males (59%), median age, 70 years), and 79 (14.7%) received calcifediol treatment. Overall, in-hospital mortality during the first 30 days was 17.5%. The OR of death for patients receiving calcifediol (mortality rate of 5%) was 0.22 (95% CI, 0.08 to 0.61) compared to patients not receiving such treatment (mortality rate of 20%; < 0.01). Patients who received calcifediol after admission were more likely than those not receiving treatment to have comorbidity and a lower rate of CURB-65 score for pneumonia severity ≥ 3 (one point for each of confusion, urea > 7 mmol/L, respiratory rate ≥ 30/min, systolic blood pressure < 90 mm Hg or diastolic blood pressure ≤ 60 mm Hg, and age ≥ 65 years), acute respiratory distress syndrome (moderate or severe), c-reactive protein, chronic kidney disease, and blood urea nitrogen. In a multivariable logistic regression model, adjusting for confounders, there were significant differences in mortality for patients receiving calcifediol compared with patients not receiving it (OR = 0.16 (95% CI 0.03 to 0.80).
Among patients hospitalized with COVID-19, treatment with calcifediol, compared with those not receiving calcifediol, was significantly associated with lower in-hospital mortality during the first 30 days. The observational design and sample size may limit the interpretation of these findings.
Calcifediol 已被提议作为 COVID-19 患者的潜在治疗方法。
比较 COVID-19 住院患者口服 Calcifediol(骨化二醇)治疗与不治疗对死亡率的影响。
回顾性、多中心、开放性、非随机队列研究。
住院治疗。
2020 年 2 月 5 日至 5 月 5 日期间,西班牙南部五家医院确诊 COVID-19 的患者。
患者接受 Calcifediol(25-羟维生素 D)治疗(0.266mg/胶囊,入院时服用 2 粒,然后第 3、7、14、21 和 28 天各服用 1 粒)或不接受治疗。
入院后 30 天内院内死亡率。
共 537 例 COVID-19 住院患者(317 例男性(59%),中位年龄 70 岁),79 例(14.7%)接受了 Calcifediol 治疗。总体而言,入院后 30 天内的院内死亡率为 17.5%。接受 Calcifediol 治疗的患者(死亡率为 5%)的死亡风险比未接受治疗的患者(死亡率为 20%)低 0.22(95%CI,0.08 至 0.61)(<0.01)。与未接受治疗的患者相比,接受 Calcifediol 治疗的患者更有可能患有合并症,肺炎严重程度 CURB-65 评分(每一项为 1 分:意识障碍、尿素 > 7mmol/L、呼吸频率 ≥ 30/min、收缩压 < 90mmHg 或舒张压 ≤ 60mmHg、年龄≥65 岁)、急性呼吸窘迫综合征(中度或重度)、C 反应蛋白、慢性肾脏病和血尿素氮的发生率较低。在多变量逻辑回归模型中,调整混杂因素后,与未接受 Calcifediol 治疗的患者相比,接受 Calcifediol 治疗的患者死亡率差异有统计学意义(OR=0.16(95%CI 0.03 至 0.80))。
在 COVID-19 住院患者中,与未接受 Calcifediol 治疗的患者相比,接受 Calcifediol 治疗与入院后 30 天内的院内死亡率显著降低相关。观察性设计和样本量可能限制了对这些发现的解释。