Zhang Xiangqun, Wu Junyuan, Dong Hongmeng, Shang Na, Li Yixuan, Zhang Ying, Guo Shubin, Mei Xue
Emergency Medicine Clinical Research Center, Beijing Chao-Yang Hospital, Capital Medical University, Beijing, China.
Beijing Key Laboratory of Cardiopulmonary Cerebral Resuscitation, Clinical Center for Medicine in Acute Infection, Capital Medical University, Beijing, China.
Front Nutr. 2024 Sep 25;11:1441847. doi: 10.3389/fnut.2024.1441847. eCollection 2024.
To analyze the impact of different methods of Vitamin D administration on the prognosis of COVID-19 patients.
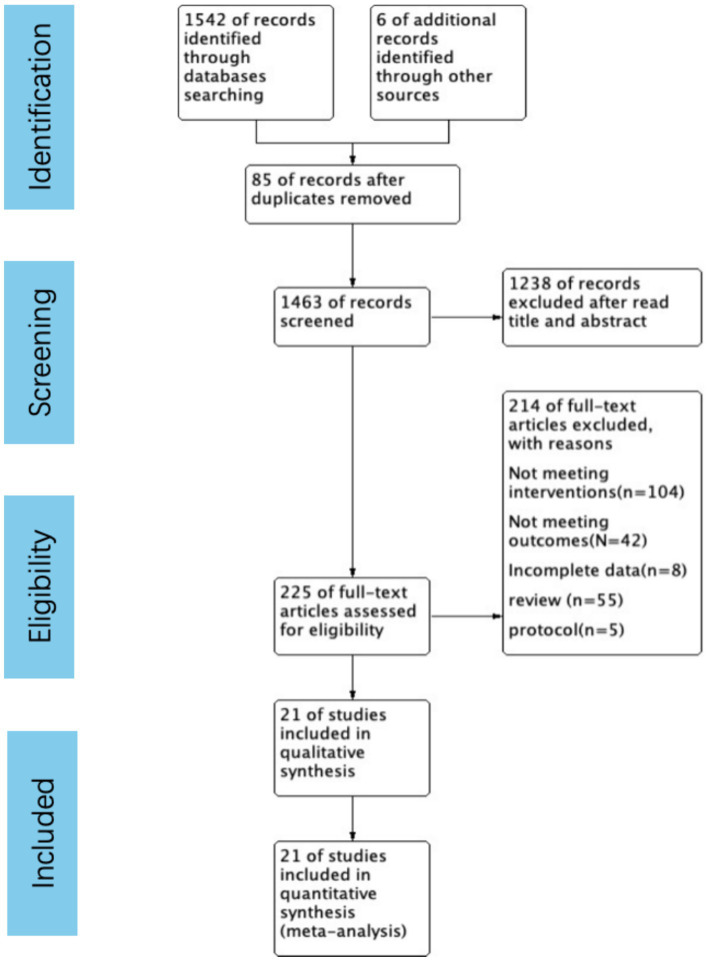
A comprehensive literature search was conducted across four databases: PubMed, Embase, Web of Science, and Cochrane, up to January 5, 2024. Eligible studies included randomized controlled trials and cohort studies that compared Vitamin D supplementation with control groups in COVID-19 patients. Outcomes of interest were mortality rate, ICU (Intensive Care Unit) admission rate, length of hospital stay, and endotracheal intubation rate. Subgroup analyses were performed based on the dosing regimen (single-dose vs. continuous-dose), total Vitamin D intake within 14 days (≥100,000 IU vs. <100,000 IU), and baseline serum Vitamin D levels (deficient group: 25OHD < 30 ng/mL vs. non-restricted group). A random-effects model was employed for meta-analysis to account for heterogeneity among studies.
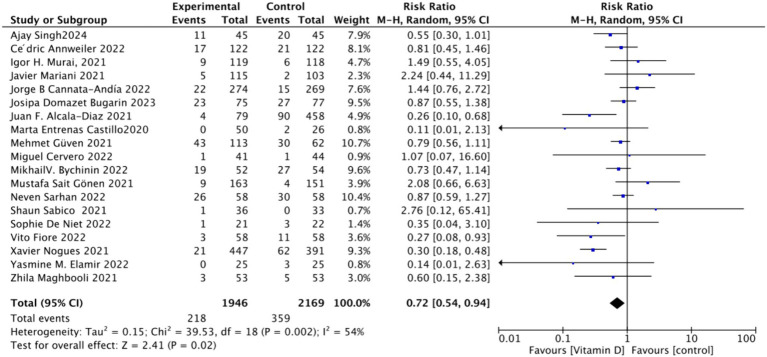
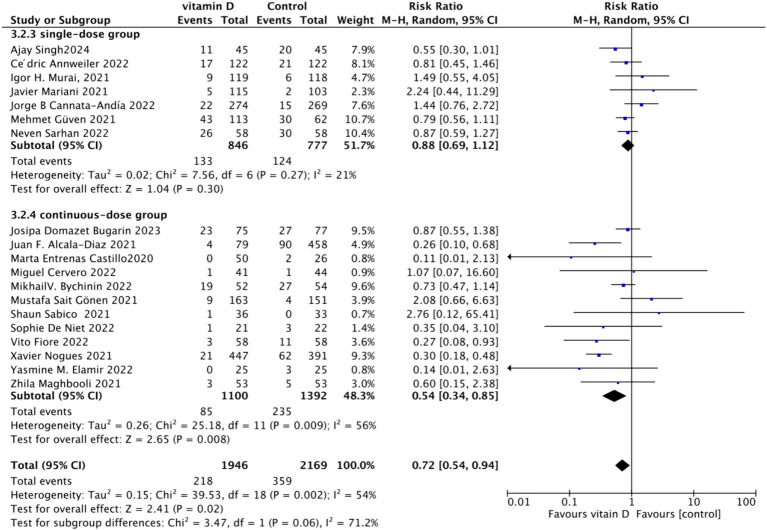
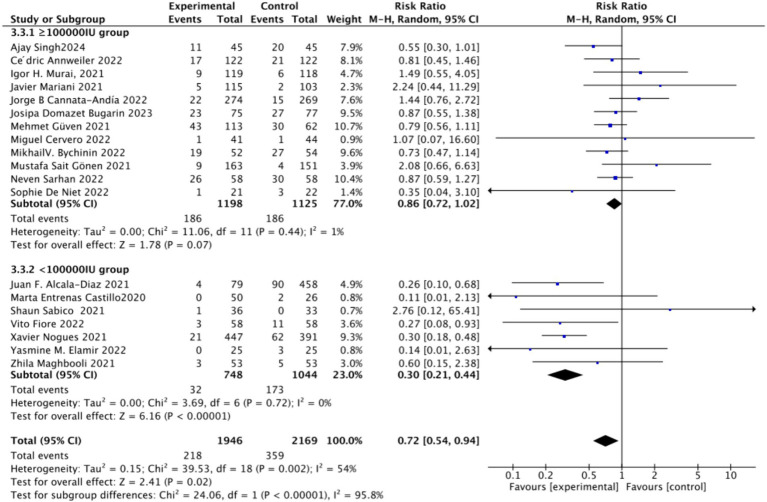
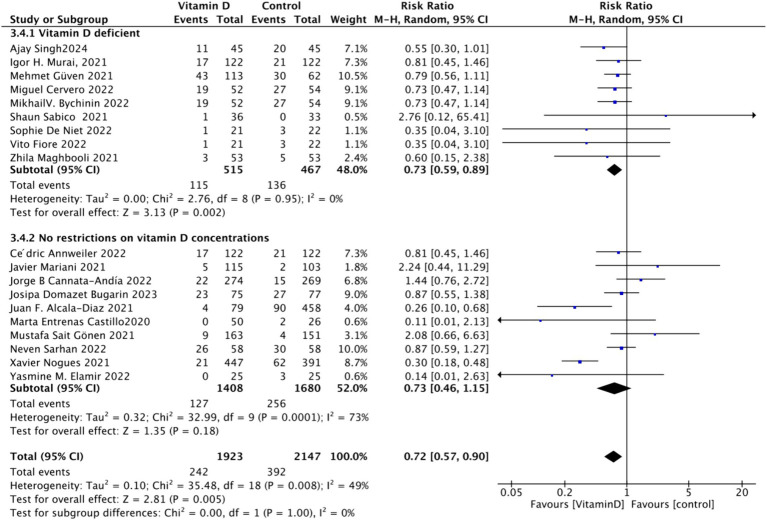
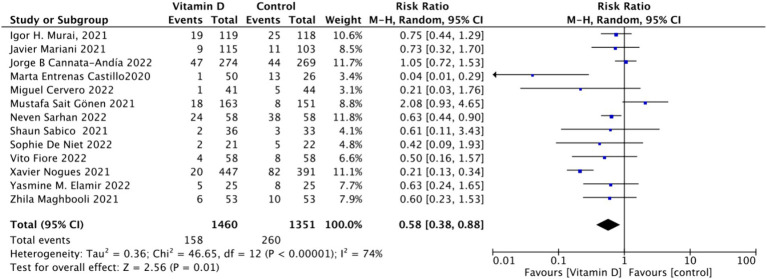
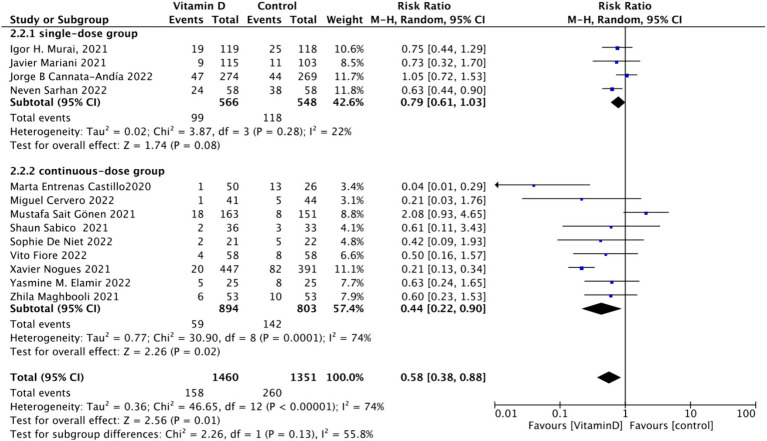
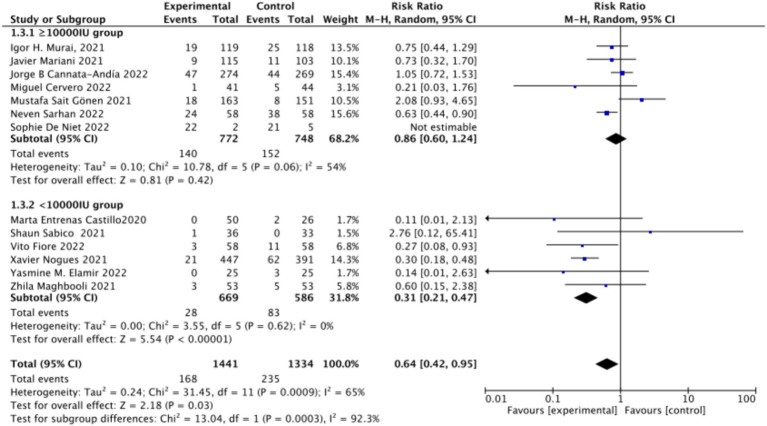
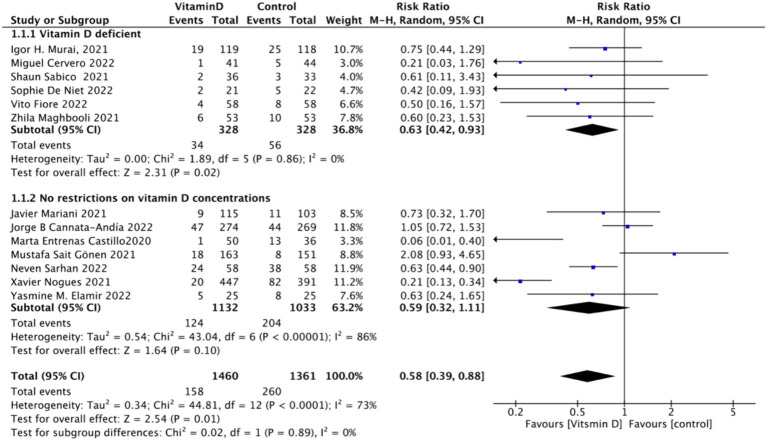
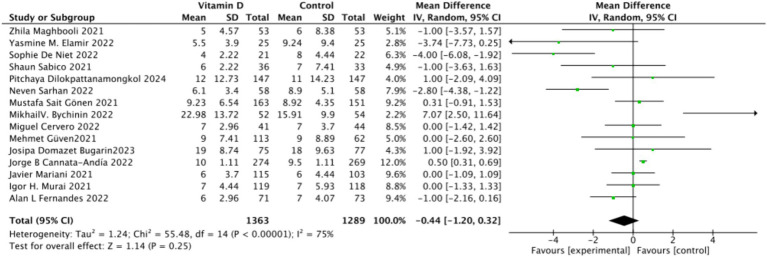
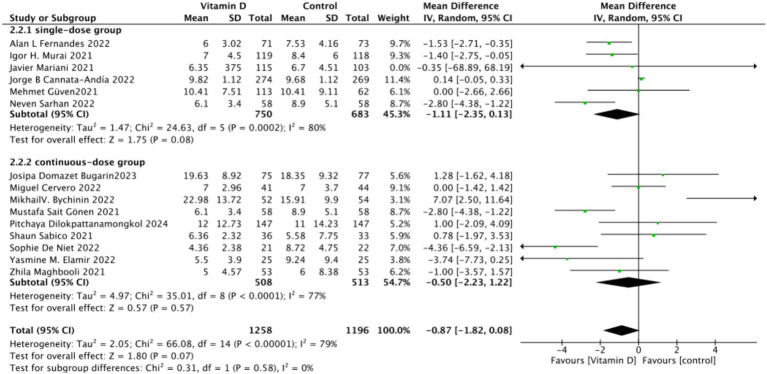
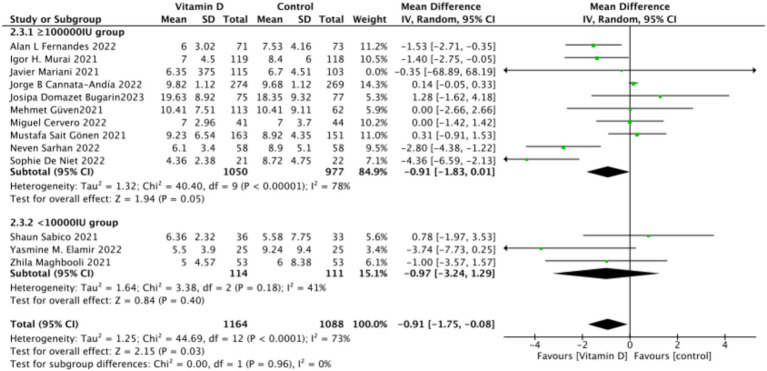
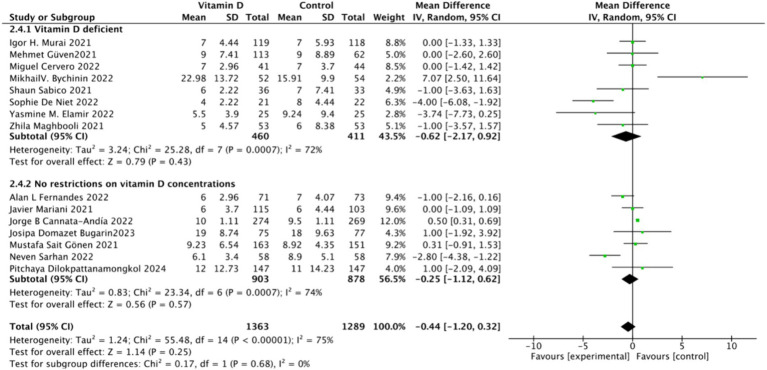
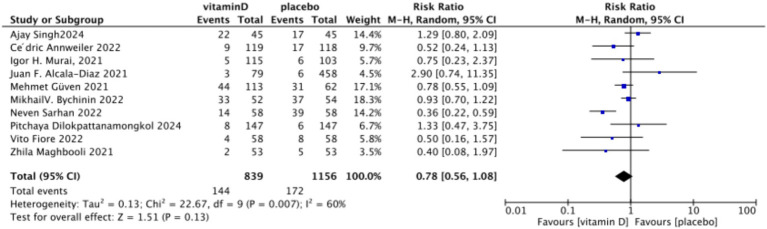
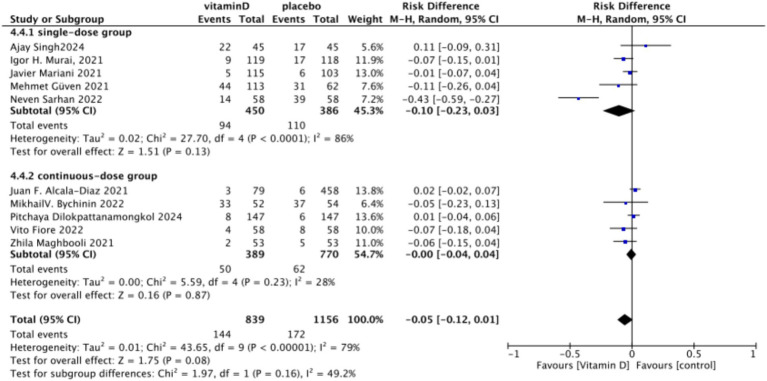
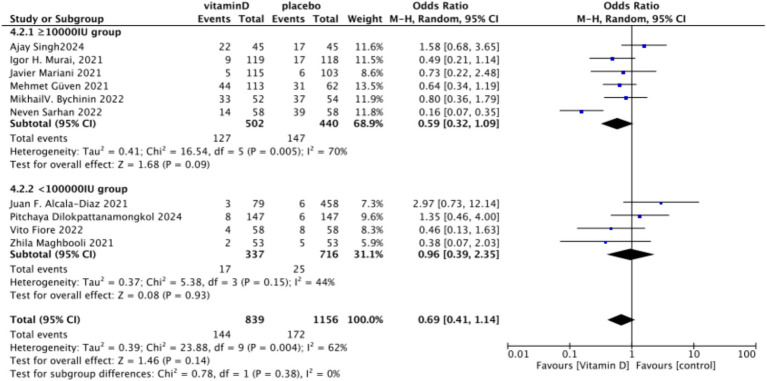
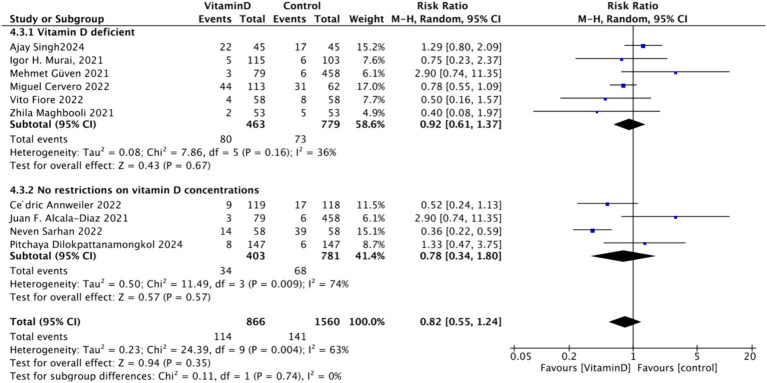
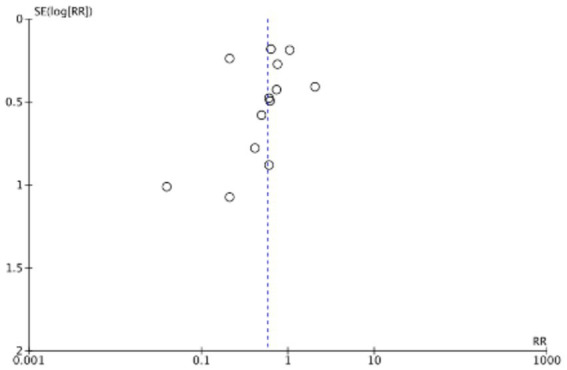
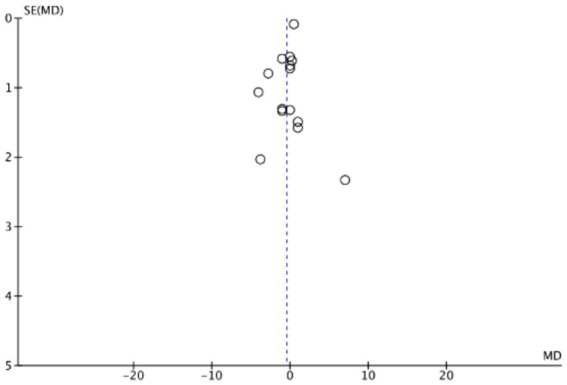
A total of 21 studies involving 4,553 participants were included. In terms of mortality, Vitamin D supplementation significantly reduced the mortality rate (RR = 0.72, 95% CI: 0.54-0.94, = 54%, = 0.02), with continuous dosing being more effective (RR = 0.53, 95% CI: 0.34-0.83, = 55%, = 0.006) compared to single-dose (RR = 0.88, 95% CI: 0.69-1.12, = 21%, = 0.3), and lower total doses (<100,000 IU) showing greater benefit (RR = 0.30, 95% CI: 0.21-0.44, = 0%, < 0.0001). Mortality was significantly reduced in the Vitamin D-deficient group (25OHD < 30 ng/mL) (RR = 0.73, 95% CI: 0.59-0.89, = 0%, = 0.002) but not in the non-restricted group. Regarding ICU admission, supplementation reduced ICU admission rates (RR = 0.58, 95% CI: 0.38-0.88, = 74%, = 0.01), with continuous dosing (RR = 0.44, 95% CI: 0.22-0.90, = 74%, = 0.02) being more effective than single-dose (RR = 0.79, 95% CI: 0.61-1.03, = 22%, = 0.08), and lower doses (<100,000 IU) providing more significant reduction (RR = 0.31, 95% CI: 0.21-0.47, = 0%, = 0.001). ICU admission rates were significantly reduced in the Vitamin D-deficient group (RR = 0.63, 95% CI: 0.42-0.93, = 0%, = 0.02) but not in the non-restricted group (RR = 0.59, 95% CI: 0.32-1.11, = 86%, = 0.1). For length of hospital stay, no significant differences were observed between Vitamin D and control groups (MD = -1, 95% CI: -2.16 to 0.16, = 0.13), and subgroup analyses by dosing regimen, total dose, and baseline Vitamin D levels also showed no significant differences. Similarly, for endotracheal intubation, there was no significant difference in intubation rates between groups (RR = 0.78, 95% CI: 0.56-1.08, = 0.13), and subgroup analyses confirmed no significant effect of different dosing strategies or baseline Vitamin D status on intubation rates.
Vitamin D supplementation improves clinical outcomes in COVID-19 patients by reducing mortality and ICU admission rates, particularly when administered continuously with a total dose of less than 100,000 IU over 14 days, and among those with baseline Vitamin D deficiency (25OHD < 30 ng/mL). However, there were no significant effects on the length of hospital stay or endotracheal intubation rates, regardless of the dosing regimen or baseline Vitamin D levels. These findings emphasize the importance of considering both the total dose over 14 days and baseline Vitamin D status to optimize therapeutic benefits.
分析不同维生素D给药方法对新型冠状病毒肺炎(COVID-19)患者预后的影响。
截至2024年1月5日,在四个数据库(PubMed、Embase、Web of Science和Cochrane)中进行了全面的文献检索。符合条件的研究包括随机对照试验和队列研究,这些研究比较了COVID-19患者补充维生素D与对照组的情况。感兴趣的结局指标为死亡率、重症监护病房(ICU)入住率、住院时间和气管插管率。根据给药方案(单剂量与连续剂量)、14天内维生素D总摄入量(≥100,000国际单位与<100,000国际单位)以及基线血清维生素D水平(缺乏组:25羟维生素D[25OHD]<30纳克/毫升与非限制组)进行亚组分析。采用随机效应模型进行荟萃分析以考虑研究间的异质性。
共纳入21项研究,涉及4553名参与者。在死亡率方面,补充维生素D显著降低了死亡率(风险比[RR]=0.72,95%置信区间[CI]:0.54 - 0.94,I²=54%,P=0.02),与单剂量给药(RR=0.88,95%CI:0.69 - 1.12,I²=21%,P=0.3)相比,连续给药更有效(RR=0.53,95%CI:0.34 - 0.83,I²=55%,P=0.006),且较低的总剂量(<100,000国际单位)显示出更大的益处(RR=0.30,95%CI:0.21 - 0.44,I²=0%,P<0.0001)。维生素D缺乏组(25OHD<30纳克/毫升)的死亡率显著降低(RR=0.73,95%CI:0.59 - 0.89,I²=0%,P=0.002),而非限制组则未降低。关于ICU入住情况,补充维生素D降低了ICU入住率(RR=0.58,95%CI:0.38 - 0.88,I²=74%,P=0.01),与单剂量给药(RR=0.79,95%CI:0.61 - 1.03,I²=22%,P=0.08)相比,连续给药(RR=0.44,95%CI:0.22 - 0.90,I²=74%,P=0.02)更有效,且较低剂量(<100,000国际单位)的降低幅度更大(RR=0.31,95%CI:0.21 - 0.47,I²=0%,P=0.001)。维生素D缺乏组的ICU入住率显著降低(RR=0.63,95%CI:0.42 - 0.93,I²=0%,P=0.02),而非限制组则未降低(RR=0.59,95%CI:0.32 - 1.11,I²=86%,P=0.1)。对于住院时间,维生素D组与对照组之间未观察到显著差异(平均差[MD]= -1,95%CI:-2.16至0.16,I²=0.13),按给药方案、总剂量和基线维生素D水平进行的亚组分析也未显示出显著差异。同样,对于气管插管,两组之间的插管率无显著差异(RR=0.78,95%CI:0.56 - 1.08,I²=0.13),亚组分析证实不同给药策略或基线维生素D状态对插管率无显著影响。
补充维生素D可通过降低死亡率和ICU入住率改善COVID-19患者的临床结局,尤其是在14天内连续给药且总剂量小于100,000国际单位时,以及在基线维生素D缺乏(25OHD<30纳克/毫升)的患者中。然而,无论给药方案或基线维生素D水平如何,对住院时间或气管插管率均无显著影响。这些发现强调了考虑14天内的总剂量和基线维生素D状态以优化治疗效果的重要性。