The Institute of Gastroenterology and Hepatology, Soroka University Medical Center and the Faculty of Health Sciences, Ben-Gurion University of the Negev, Beer-Sheva, Israel.
Department of Gastroenterology and Hepatology, Hadassah Hebrew University Medical Center, Jerusalem, Israel.
United European Gastroenterol J. 2021 Jul;9(6):681-687. doi: 10.1002/ueg2.12106. Epub 2021 Jun 2.
Recently, three updated guidelines for post-polypectomy colonoscopy surveillance (PPCS) have been published. These guidelines are based on a comprehensive summary of the literature, while some recommendations are similar, different surveillance intervals are recommended after detection of specific types of polyps.
In this review, we aimed to compare and contrast these recommendations.
The updated guidelines for PPCS were reviewed and the recommendations were compared.
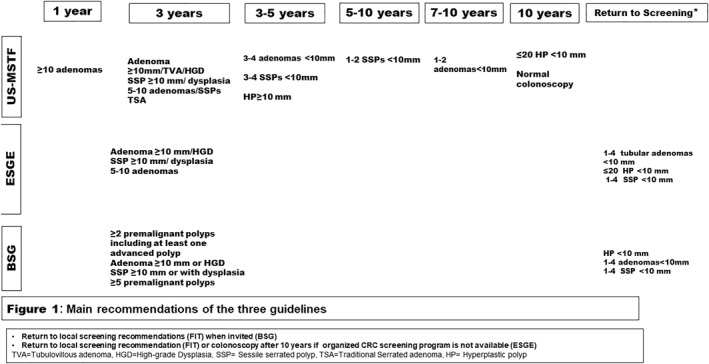
For patients with 1-4 adenomas <10 mm with low-grade dysplasia, irrespective of villous components, or 1-4 serrated polyps <10 mm without dysplasia, the European Society of Gastrointestinal Endoscopy (ESGE) and British Society of Gastroenterology (BSG), the Association of Coloproctology of Great Britain and Ireland (ACPGBI) and Public Health England (PHE) (BSG/ACPGBI/PHE) guidelines do not recommend colonoscopic surveillance and instead recommend that the participate in routine CRC screening program (typically based on the fecal immunochemical test), while the USMSTF recommends surveillance colonoscopies 7-10 years after diagnosis of 1-2 tubular adenomas <10 mm and 3-5 years for 3-4 tubular adenomas of the same size. The USMSTF define adenomas with tubulovillous or villous histology as high-risk adenomas; thus, surveillance colonoscopy is recommended after 3 years. However, the ESGE and BSG do not consider such histology as a criterion for repeating colonoscopy at this short interval. For patients with 1-2 sessile serrated polyps (SSPs) <10 mm and those with 3-4 SSPs <10 mm, the USMSTF recommends surveillance colonosocopy after 5-10 and 3-5 years, respectively.
最近,发布了三项更新的息肉切除术后结肠镜检查监测(PPCS)指南。这些指南是基于对文献的全面总结,虽然一些建议相似,但对于检测到特定类型息肉后的监测间隔时间,不同指南推荐有所不同。
在本综述中,我们旨在比较和对比这些建议。
审查了 PPCS 的更新指南,并对建议进行了比较。
对于直径<10mm、低级别不典型增生的 1-4 个无蒂腺瘤或<10mm 无不典型增生锯齿状息肉的患者,欧洲胃肠道内镜学会(ESGE)和英国胃肠病学会(BSG)、英国和爱尔兰结直肠学会(ACPGBI)和英格兰公共卫生署(PHE)(BSG/ACPGBI/PHE)指南不建议进行结肠镜监测,而建议参加常规结直肠癌筛查计划(通常基于粪便免疫化学测试),而美国多学会息肉切除术后监测工作组(USMSTF)建议对 1-2 个直径<10mm 的管状腺瘤和 3-4 个相同大小的管状腺瘤进行 7-10 年和 3-5 年的监测结肠镜检查。USMSTF 将具有管状绒毛或绒毛状组织学的腺瘤定义为高危腺瘤;因此,建议在 3 年后进行监测结肠镜检查。然而,ESGE 和 BSG 并不认为这种组织学是在如此短的时间间隔内重复结肠镜检查的标准。对于直径<10mm 的 1-2 个无蒂锯齿状息肉(SSP)和 3-4 个直径<10mm 的 SSP 患者,USMSTF 建议分别在 5-10 年和 3-5 年后进行监测结肠镜检查。