Stroke Unit and Clinical Neurology, Department of Neuroscience, Udine University Hospital, Piazzale S. Maria della Misericordia 15, 33100, Udine, Italy.
Clinical Neurology, Udine University Hospital, Udine, Italy.
Sci Rep. 2021 Jun 2;11(1):11634. doi: 10.1038/s41598-021-91257-5.
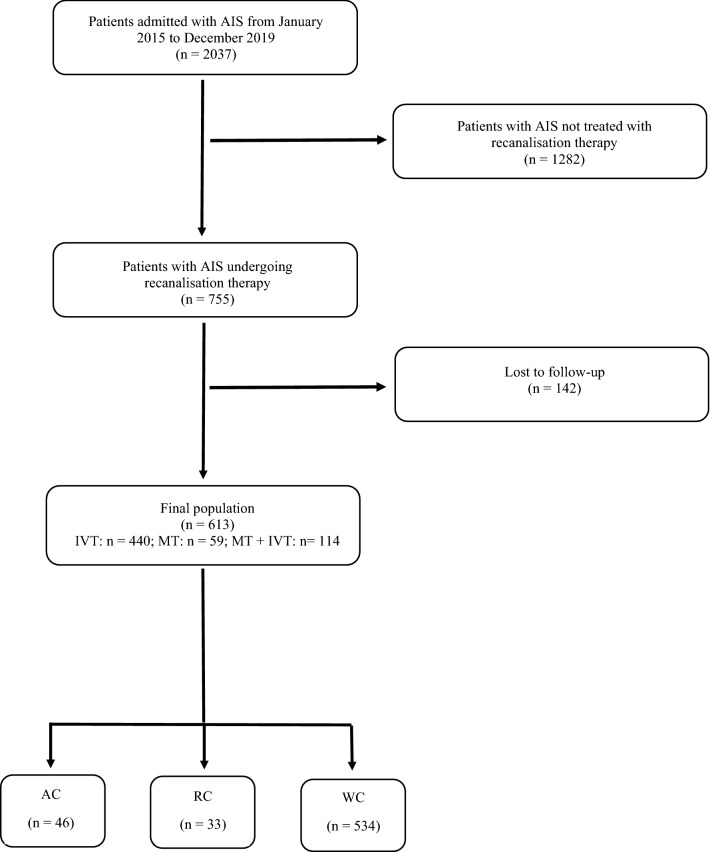
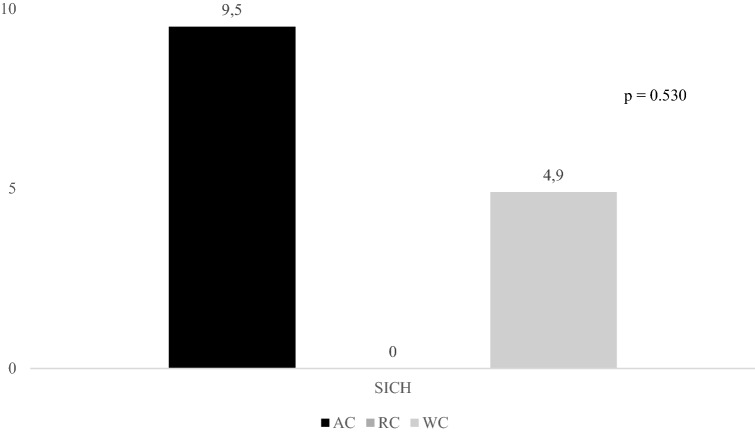
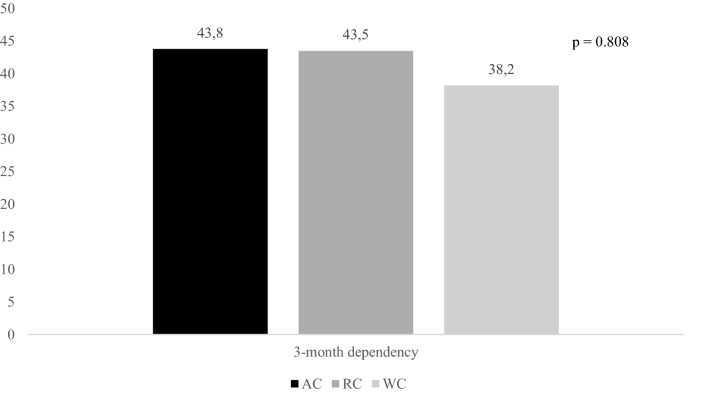
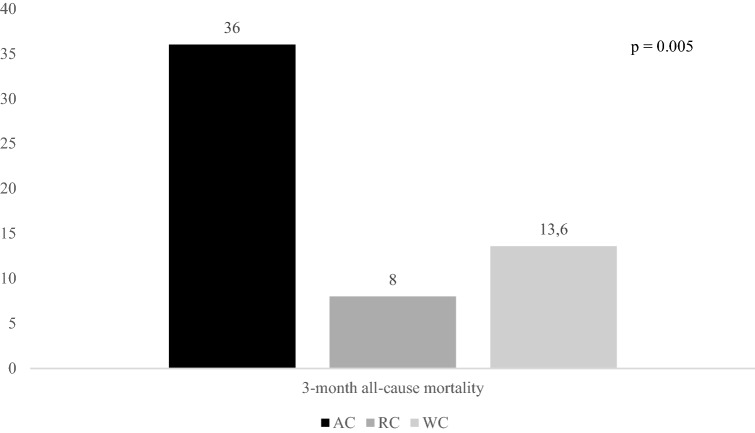
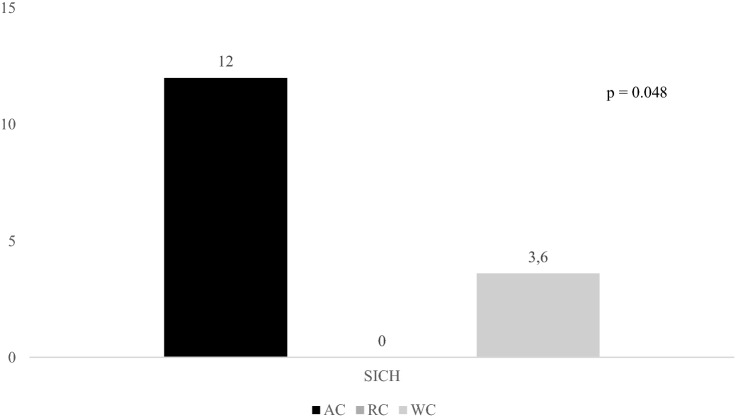
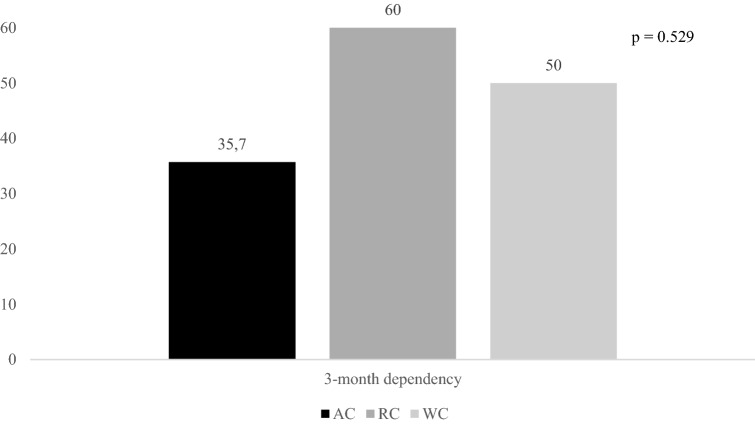
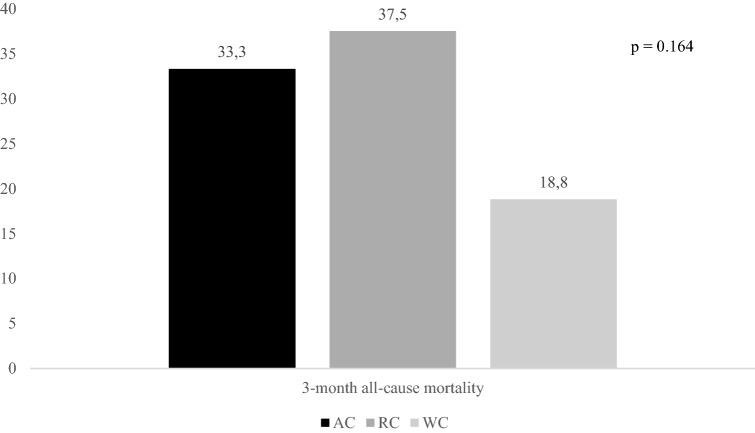
To date, very few studies focused their attention on efficacy and safety of recanalisation therapy in acute ischemic stroke (AIS) patients with cancer, reporting conflicting results. We retrospectively analysed data from our database of consecutive patients admitted to the Udine University Hospital with AIS that were treated with recanalisation therapy, i.e. intravenous thrombolysis (IVT), mechanical thrombectomy (MT), and bridging therapy, from January 2015 to December 2019. We compared 3-month dependency, 3-month mortality, and symptomatic intracranial haemorrhage (SICH) occurrence of patients with active cancer (AC) and remote cancer (RC) with that of patients without cancer (WC) undergoing recanalisation therapy for AIS. Patients were followed up for 3 months. Among the 613 AIS patients included in the study, 79 patients (12.9%) had either AC (n = 46; 7.5%) or RC (n = 33; 5.4%). Although AC patients, when treated with IVT, had a significantly increased risk of 3-month mortality [odds ratio (OR) 6.97, 95% confidence interval (CI) 2.42-20.07, p = 0.001] than WC patients, stroke-related deaths did not differ between AC and WC patients (30% vs. 28.8%, p = 0.939). There were no significant differences between AC and WC patients, when treated with MT ± IVT, regarding 3-month dependency, 3-month mortality and SICH. Functional independence, mortality, and SICH were similar between RC and WC patients. In conclusion, recanalisation therapy might be used in AIS patients with nonmetastatic AC and with RC. Further studies are needed to explore the outcome of AIS patients with metastatic cancer undergoing recanalisation therapy.
迄今为止,很少有研究关注癌症合并急性缺血性卒中(AIS)患者的再通治疗的疗效和安全性,且结果相互矛盾。我们回顾性分析了 2015 年 1 月至 2019 年 12 月期间连续入住乌迪内大学医院的 AIS 患者的数据库数据,这些患者接受了再通治疗,包括静脉溶栓(IVT)、机械血栓切除术(MT)和桥接治疗。我们比较了接受 AIS 再通治疗的有活动性癌症(AC)和转移性癌症(RC)患者与无癌症(WC)患者的 3 个月依赖性、3 个月死亡率和症状性颅内出血(SICH)发生率。患者接受了 3 个月的随访。在纳入研究的 613 名 AIS 患者中,79 名患者(12.9%)患有 AC(n=46;7.5%)或 RC(n=33;5.4%)。尽管 AC 患者在接受 IVT 治疗时,3 个月死亡率的风险显著增加[比值比(OR)6.97,95%置信区间(CI)2.42-20.07,p=0.001],但 AC 患者与 WC 患者的卒中相关死亡率无差异(30%比 28.8%,p=0.939)。当接受 MT±IVT 治疗时,AC 患者与 WC 患者在 3 个月依赖性、3 个月死亡率和 SICH 方面无显著差异。RC 患者与 WC 患者的功能独立性、死亡率和 SICH 相似。总之,非转移性 AC 和 RC 的 AIS 患者可以使用再通治疗。需要进一步研究来探讨接受再通治疗的转移性癌症合并 AIS 患者的结局。