Departments of Physical Therapy and Athletic Training (J.A.Z., T.B., T.R.D., T.N., T.D.E) and Occupational Therapy (D.F.), Sargent College of Health and Rehabilitation Sciences, Boston University, Boston, Massachusetts; Department of Physical Therapy (J.T.C.), University of New England, Portland, Maine; Department of Kinesiology (C.C.-S.), College of Agriculture, Health, and Natural Resources, University of Connecticut, Storrs, Connecticut; Program in Physical Therapy (R.P.D., K.S.R., G.M.E), Department of Neuroscience (G.M.E), and Department of Neurology (R.P.D., G.M.E), Washington University in St Louis School of Medicine, St Louis, Missouri; School of Public Health (M.L.), Boston University, Boston, Massachusetts; and Department of Neurology (M.S.-H., C.A.T.), Parkinson's Disease and Movement Disorders Center, Boston University, Boston, Massachusetts.
J Neurol Phys Ther. 2021 Oct 1;45(4):259-265. doi: 10.1097/NPT.0000000000000362.
Walking activity in persons with Parkinson disease (PD) is important for preventing functional decline. The contribution of walking activity to home and community mobility in PD is poorly understood.
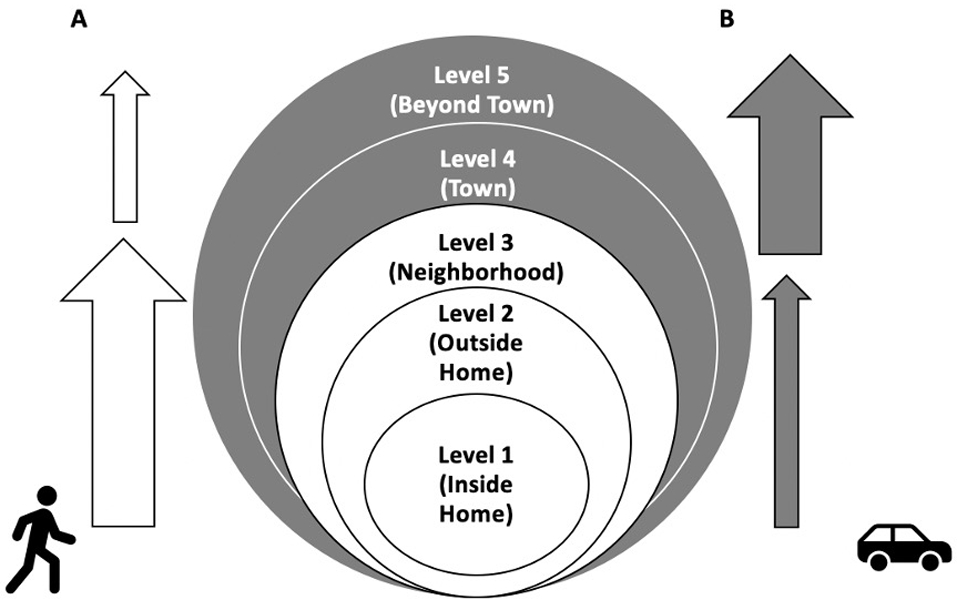
Cross-sectional baseline data (N = 69) were analyzed from a randomized controlled PD trial. The Life-Space Assessment (LSA) quantified the extent, frequency, and independence across 5 expanding levels of home and community mobility, producing individual subscores and a total score. Two additional summed scores were used to represent mobility within (Levels 1-3) and beyond (Levels 4-5) neighborhood limits. An accelerometer measured walking activity for 7 days. Regression and correlation analyses evaluated relationships between daily steps and mobility scores. Mann-Whitney U tests secondarily compared differences in mobility scores between the active and sedentary groups.
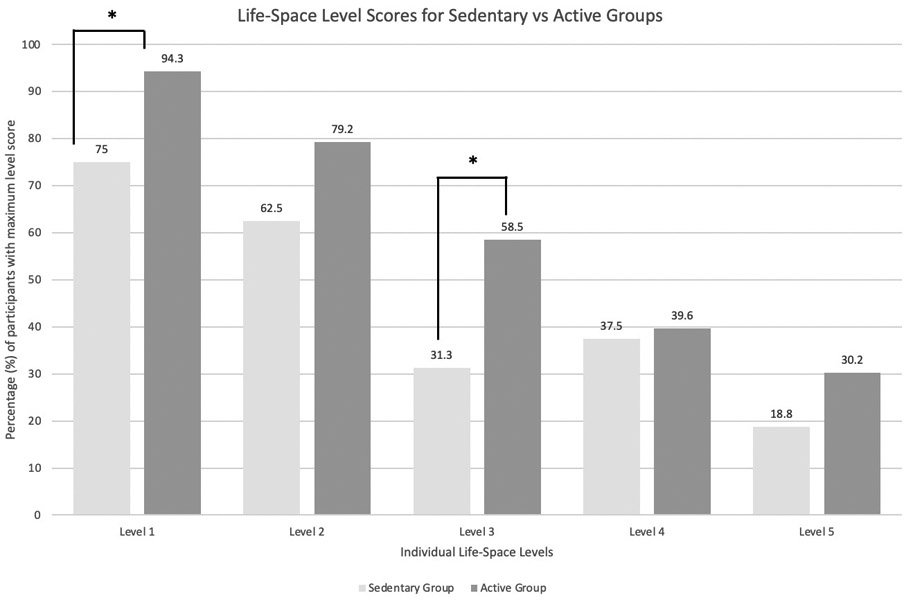
Walking activity contributed significantly to the summed Level 1-3 score (β = 0.001, P = 0.004) but not to the summed Level 4-5 (β = 0.001, P = 0.33) or total (β = 0.002, P = 0.07) scores. Walking activity was significantly related to Level 1 (ρ = 0.336, P = 0.005), Level 2 (ρ = 0.307, P = 0.010), and Level 3 (ρ = 0.314, P = 0.009) subscores. Only the summed Level 1-3 score (P = 0.030) was significantly different between the active and sedentary groups.
Persons with PD who demonstrated greater mobility beyond the neighborhood were not necessarily more active; walking activity contributed more so to home and neighborhood mobility. Compared with LSA total score, the Level 1-3 summed score may be a more useful participation-level measure for assessing the impact of changes in walking activity.Video Abstract available for more insights from the authors (see the Video, Supplemental Digital Content 1 available at: http://links.lww.com/JNPT/A349).
帕金森病(PD)患者的步行活动对预防功能下降很重要。步行活动对 PD 患者居家和社区移动能力的贡献尚不清楚。
对一项随机对照 PD 试验的横断面基线数据(N=69)进行了分析。生活空间评估(LSA)量化了 5 个扩展水平的居家和社区移动范围的程度、频率和独立性,产生了个体子分数和总分数。另外两个加分数用于代表邻里限制内(水平 1-3)和超越(水平 4-5)的移动能力。加速度计连续 7 天测量步行活动。回归和相关分析评估了每日步数与移动能力评分之间的关系。曼-惠特尼 U 检验其次比较了活跃组和久坐组之间移动能力评分的差异。
步行活动对总和 1-3 分(β=0.001,P=0.004)有显著贡献,但对总和 4-5 分(β=0.001,P=0.33)或总和(β=0.002,P=0.07)无显著贡献。步行活动与水平 1(ρ=0.336,P=0.005)、水平 2(ρ=0.307,P=0.010)和水平 3(ρ=0.314,P=0.009)子分数有显著关系。只有总和 1-3 分(P=0.030)在活跃组和久坐组之间有显著差异。
表现出超越邻里范围更大移动能力的 PD 患者不一定更活跃;步行活动对居家和邻里移动能力的贡献更大。与 LSA 总分相比,总和 1-3 分可能是评估步行活动变化对参与度影响的更有用的指标。视频摘要可供作者提供更多见解(见视频,补充数字内容 1 可在以下网址获得:http://links.lww.com/JNPT/A349)。