US Acute Care Solutions, Canton, OH; Department of Emergency Medicine, Allegheny Health Network, Pittsburgh, PA.
Department of Health Policy, The Heller School for Social Policy and Management, Brandeis University, Waltham, MA.
Ann Emerg Med. 2021 Oct;78(4):487-499. doi: 10.1016/j.annemergmed.2021.04.026. Epub 2021 Apr 27.
We describe how the coronavirus disease 2019 (COVID-19) pandemic affected the economics of emergency department care (ED).
We conducted an observational study of 136 EDs from January 2019 to September 2020, using 2020-to-2019 3-week moving ratios for ED visits, complexity, revenue, and staffing expenses. We tabulated 2020-to-2019 staffing ratios and calculated hour and full-time-equivalent changes.
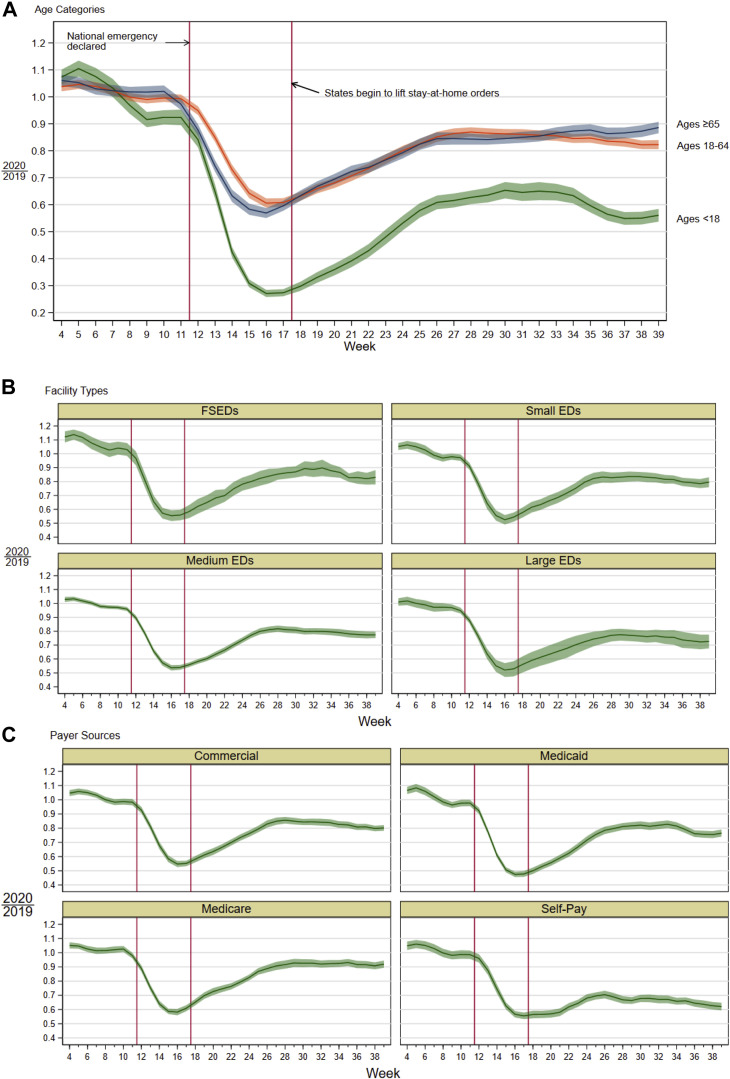
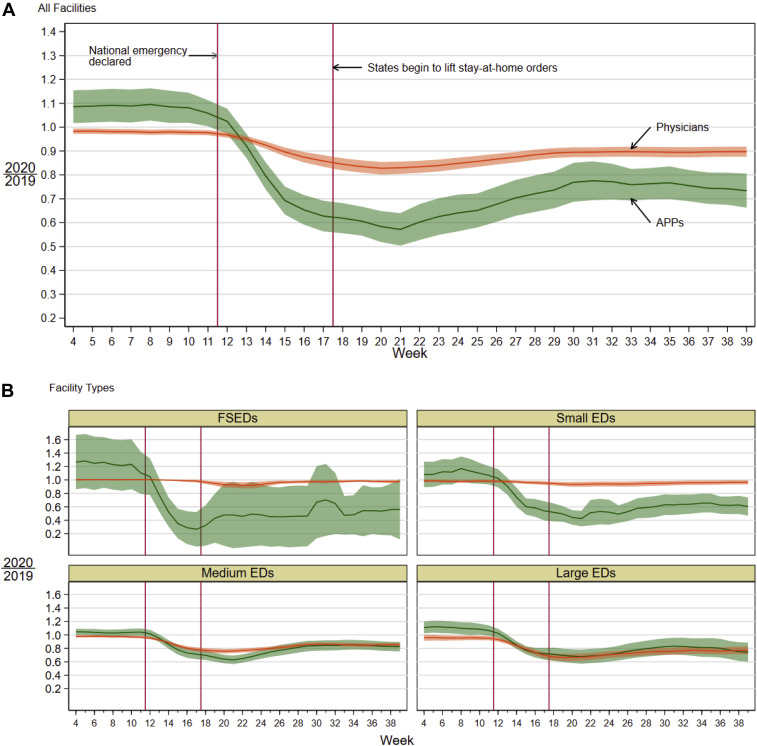
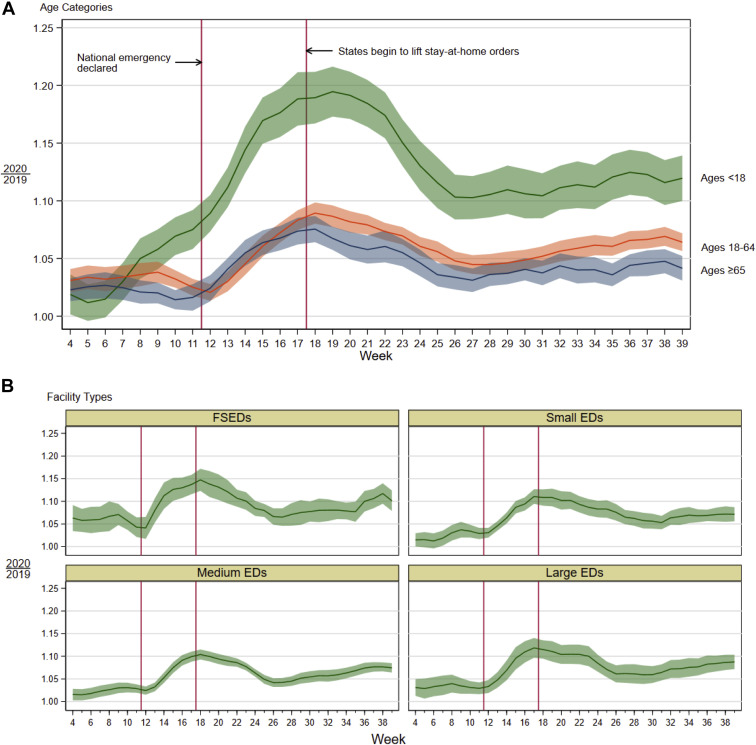
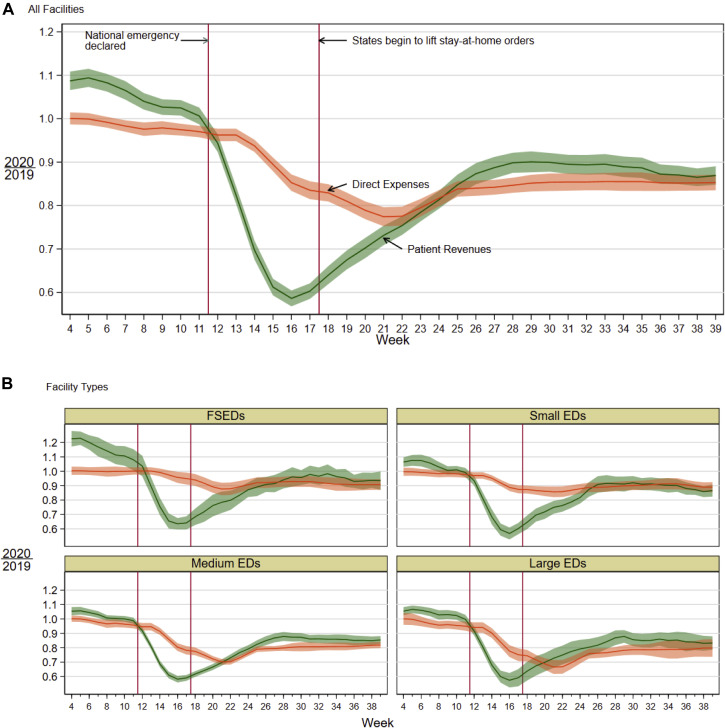
Following the COVID-19 pandemic's onset, geriatric (age ≥65), adult (age 18 to 64), and pediatric (age <18) ED visits declined by 43%, 40%, and 73%, respectively, compared to 2019 visits and rose thereafter but remained below 2019 levels through September. Relative value units per visit rose by 8%, 9%, and 18%, respectively, compared to 2019, while ED admission rates rose by 32%. Both fell subsequently but remained above 2019 levels through September. Revenues dropped sharply early in the pandemic and rose gradually but remained below 2019 levels. In medium and large EDs, staffing and expenses were lowered with a lag, largely compensating for lower revenue at these sites, and barely at freestanding EDs. Staffing and expense reductions could not match revenue losses in smaller EDs. During the pandemic, emergency physician and advanced practice provider clinical hours and compensation fell 15% and 27%, respectively, corresponding to 174 lost physician and 193 lost advanced practice provider full-time-equivalent positions.
The COVID-19 pandemic adversely impacted the economics of ED care, with large drops in overall and, in particular, low-acuity ED visits, necessitating reductions in clinical hours. Staffing cutbacks could not match reduced revenue at small EDs with minimum emergency physician coverage requirements.
我们描述了 2019 年冠状病毒病(COVID-19)大流行如何影响急诊部门护理(ED)的经济学。
我们对 2019 年 1 月至 2020 年 9 月的 136 家急诊室进行了一项观察性研究,使用 ED 就诊、复杂性、收入和人员配置费用的 2020-2019 年 3 周移动比率。我们列出了 2020-2019 年的人员配置比率,并计算了小时和全职等效变化。
COVID-19 大流行开始后,老年(年龄≥65 岁)、成人(年龄 18 至 64 岁)和儿科(年龄<18 岁)急诊就诊量分别比 2019 年就诊量下降了 43%、40%和 73%,此后有所上升,但直到 9 月仍低于 2019 年的水平。与 2019 年相比,每次就诊的相对价值单位分别增加了 8%、9%和 18%,而 ED 入院率上升了 32%。随后两者均有所下降,但截至 9 月仍高于 2019 年的水平。大流行早期收入急剧下降,随后逐渐上升,但仍低于 2019 年的水平。在中型和大型急诊室,人员配置和费用滞后降低,主要是为了弥补这些地点的收入较低,勉强维持了独立急诊室的运营。较小的急诊室无法通过减少人员配置和费用来弥补收入损失。在大流行期间,急诊医师和高级执业医师的临床工作时间和薪酬分别下降了 15%和 27%,相当于损失了 174 个急诊医师和 193 个高级执业医师全职等效职位。
COVID-19 大流行对 ED 护理的经济学产生了不利影响,总体就诊量大幅下降,特别是低 acuity ED 就诊量大幅下降,需要减少临床工作时间。小型急诊室的人员削减无法与收入减少相匹配,这些急诊室需要最低数量的急诊医师来保证基本运营。