Hong Duo, Zhang Lina, Xu Ke, Wan Xiaoting, Guo Yan
Department of Radiology, The First Hospital of China Medical University, Shenyang, China.
GE Healthcare, Beijing, China.
Front Oncol. 2021 May 28;11:628982. doi: 10.3389/fonc.2021.628982. eCollection 2021.
The purpose of this study was to investigate the prognostic value of pre-treatment CT radiomics and clinical factors for the overall survival (OS) of advanced (IIIB-IV) lung adenocarcinoma patients.
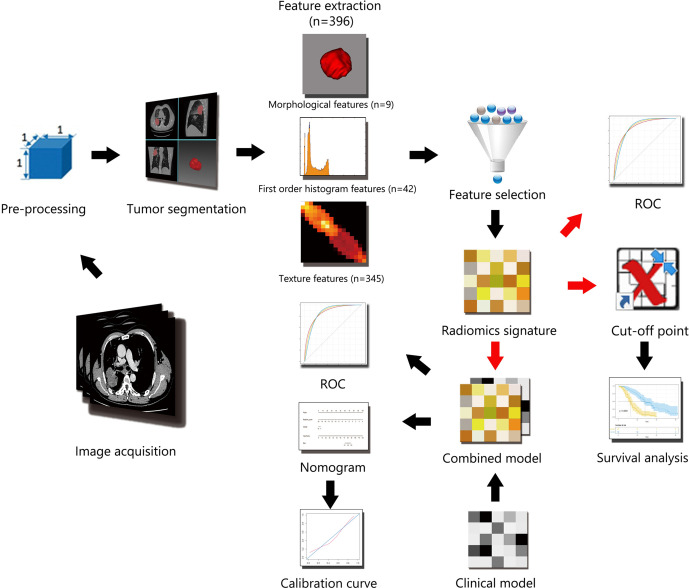
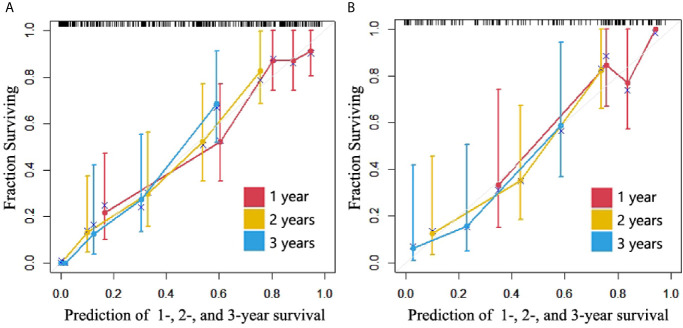
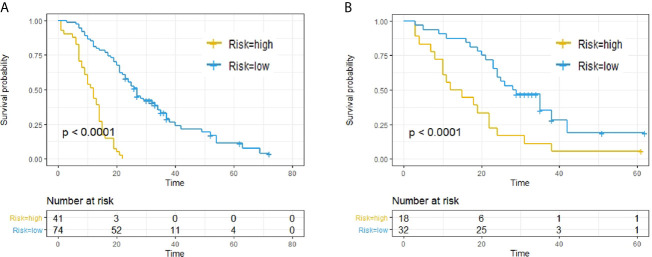
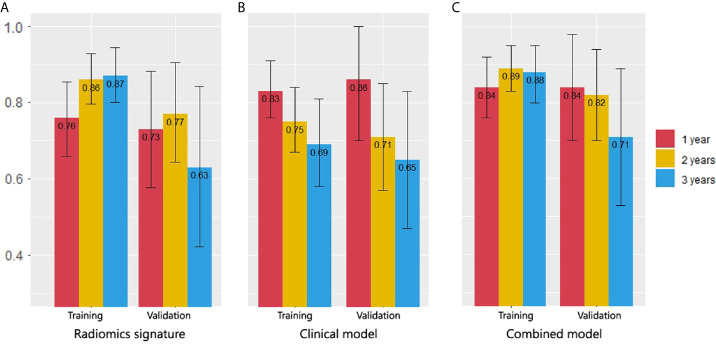
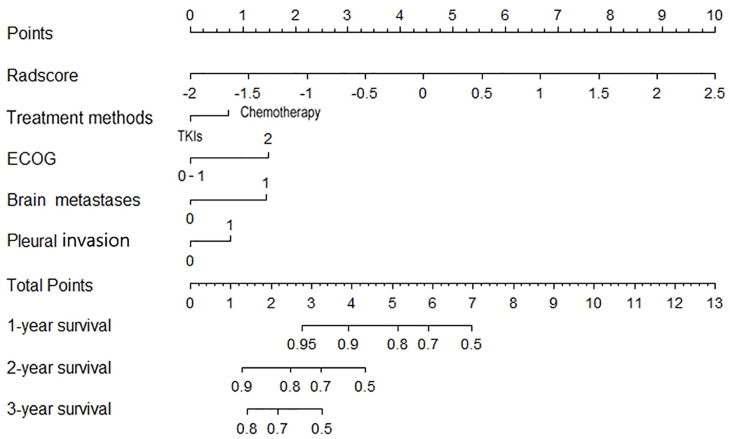
This study involved 165 patients with advanced lung adenocarcinoma. The Lasso-Cox regression model was used for feature selection and radiomics signature building. Then a clinical model was built based on clinical factors; a combined model in the form of nomogram was constructed with both clinical factors and the radiomics signature. Harrell's concordance index (C-Index) and Receiver operating characteristic (ROC) curves at cut-off time points of 1-, 2-, and 3- year were used to estimate and compare the predictive ability of all three models. Finally, the discriminatory ability and calibration of the nomogram were analyzed.
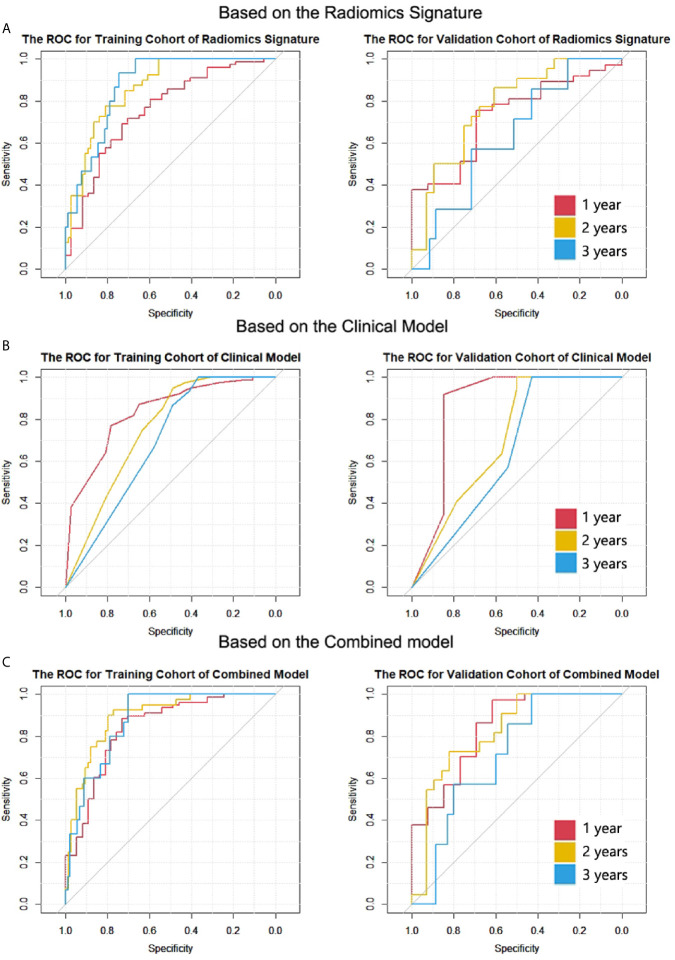
Thirteen significant features were selected to build the radiomics signature whose C-indexes were 0.746 (95% CI, 0.699 to 0.792) in the training cohort and 0.677 (95% CI, 0.597 to 0.766) in the validation cohort. The C-indexes of combined model achieved 0.799 (95% CI, 0.757 to 0.84) in the training cohort and 0.733 (95% CI, 0.656 to 0.81) in the validation cohort, which outperformed the clinical model and radiomics signature. Moreover, the areas under the curve (AUCs) of the radiomic signature for 2-year prediction was superior to that of the clinical model. The combined model had the best AUCs for 2- and 3-year predictions.
Radiomic signatures and clinical factors have prognostic value for OS in advanced (IIIB-IV) lung adenocarcinoma patients. The optimal model should be selected according to different cut-off time points in clinical application.
本研究旨在探讨治疗前CT影像组学和临床因素对晚期(IIIB-IV期)肺腺癌患者总生存期(OS)的预后价值。
本研究纳入了165例晚期肺腺癌患者。采用Lasso-Cox回归模型进行特征选择和影像组学特征构建。然后基于临床因素建立临床模型;将临床因素和影像组学特征构建成列线图形式的联合模型。使用Harrell一致性指数(C指数)以及1年、2年和3年截断时间点的受试者操作特征(ROC)曲线来估计和比较这三种模型的预测能力。最后,分析列线图的鉴别能力和校准情况。
选择了13个显著特征来构建影像组学特征,其在训练队列中的C指数为0.746(95%CI,0.699至0.792),在验证队列中的C指数为0.677(95%CI,0.597至0.766)。联合模型在训练队列中的C指数达到0.799(95%CI,0.757至0.84),在验证队列中的C指数为0.733(95%CI,0.656至0.81),优于临床模型和影像组学特征。此外,影像组学特征用于2年预测的曲线下面积(AUC)优于临床模型。联合模型在2年和3年预测中具有最佳的AUC。
影像组学特征和临床因素对晚期(IIIB-IV期)肺腺癌患者的OS具有预后价值。在临床应用中,应根据不同的截断时间点选择最佳模型。