Division of Endocrinology and Metabolism, Department of Medicine, University of Virginia School of Medicine, Charlottesville, VA.
Center for Advanced Medical Analytics, University of Virginia, Charlottesville, VA.
Crit Care Med. 2022 Mar 1;50(3):e221-e230. doi: 10.1097/CCM.0000000000005171.
We tested the hypothesis that routine monitoring data could describe a detailed and distinct pathophysiologic phenotype of impending hypoglycemia in adult ICU patients.
Retrospective analysis leading to model development and validation.
All ICU admissions wherein patients received insulin therapy during a 4-year period at the University of Virginia Medical Center. Each ICU was equipped with continuous physiologic monitoring systems whose signals were archived in an electronic data warehouse along with the entire medical record.
Eleven thousand eight hundred forty-seven ICU patient admissions.
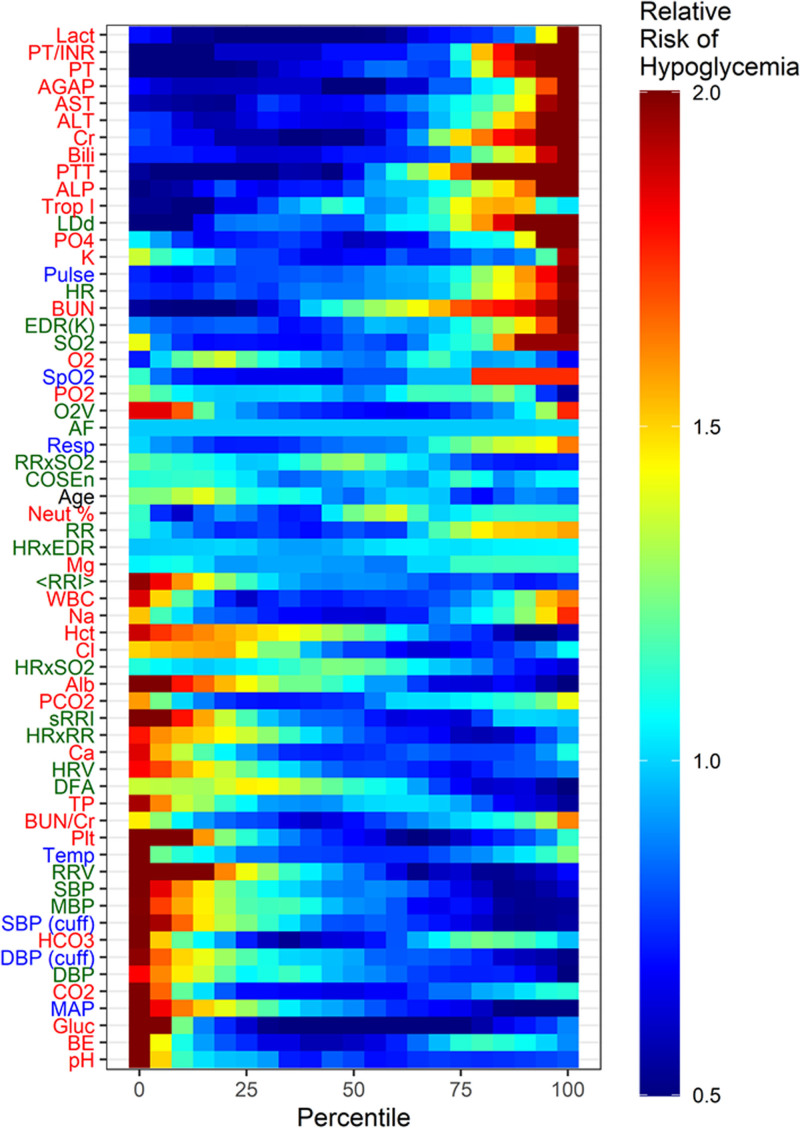
The primary outcome was hypoglycemia, defined as any episode of blood glucose less than 70 mg/dL where 50% dextrose injection was administered within 1 hour. We used 61 physiologic markers (including vital signs, laboratory values, demographics, and continuous cardiorespiratory monitoring variables) to inform the model.
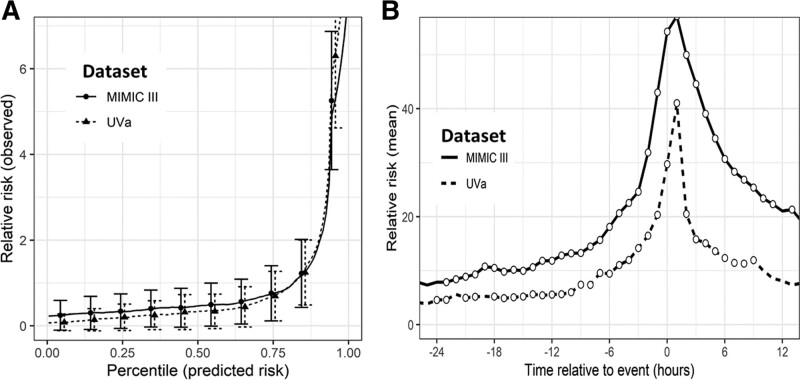
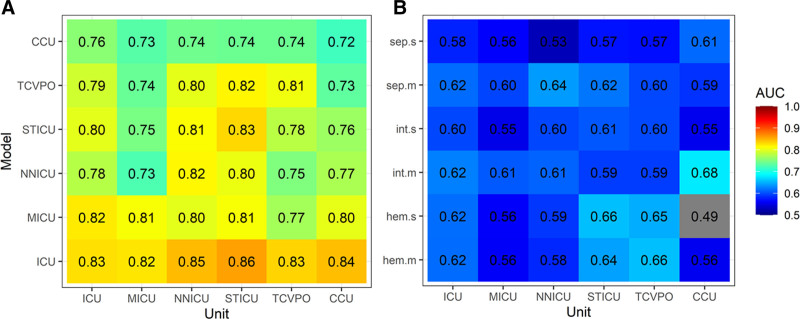
Our dataset consisted of 11,847 ICU patient admissions, 721 (6.1%) of which had one or more hypoglycemic episodes. Multivariable logistic regression analysis revealed a pathophysiologic signature of 41 independent variables that best characterized ICU hypoglycemia. The final model had a cross-validated area under the receiver operating characteristic curve of 0.83 (95% CI, 0.78-0.87) for prediction of impending ICU hypoglycemia. We externally validated the model in the Medical Information Mart for Intensive Care III critical care dataset, where it also demonstrated good performance with an area under the receiver operating characteristic curve of 0.79 (95% CI, 0.77-0.81).
We used data from a large number of critically ill inpatients to develop and externally validate a predictive model of impending ICU hypoglycemia. Future steps include incorporating this model into a clinical decision support system and testing its effects in a multicenter randomized controlled clinical trial.
我们检验了一个假设,即常规监测数据可以描述成人 ICU 患者即将发生低血糖的详细而独特的病理生理表型。
回顾性分析导致模型开发和验证。
弗吉尼亚大学医疗中心在 4 年期间所有接受胰岛素治疗的 ICU 入院患者。每个 ICU 都配备了连续的生理监测系统,其信号与整个医疗记录一起存储在电子数据仓库中。
11847 名 ICU 患者入院。
主要结局是低血糖,定义为任何一次血糖低于 70mg/dL,其中 50%葡萄糖注射液在 1 小时内给予。我们使用了 61 个生理标志物(包括生命体征、实验室值、人口统计学和连续心肺监测变量)来为模型提供信息。
我们的数据集包括 11847 名 ICU 患者入院,其中 721 名(6.1%)有一次或多次低血糖发作。多变量逻辑回归分析揭示了 41 个独立变量的病理生理特征,这些特征最好地描述了 ICU 低血糖。最终模型在接受者操作特征曲线下的交叉验证面积为 0.83(95%置信区间,0.78-0.87),用于预测即将发生的 ICU 低血糖。我们在医疗信息集市 III 重症监护数据集外部验证了该模型,该模型在接受者操作特征曲线下的面积也表现出良好的性能,为 0.79(95%置信区间,0.77-0.81)。
我们使用大量危重病患者的数据开发并外部验证了一个即将发生的 ICU 低血糖预测模型。未来的步骤包括将该模型纳入临床决策支持系统,并在多中心随机对照临床试验中测试其效果。