Department of Medical Oncology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China.
Thorac Cancer. 2021 Aug;12(16):2233-2240. doi: 10.1111/1759-7714.14057. Epub 2021 Jun 28.
Previous studies have demonstrated the combination of epidermal growth factor receptor (EGFR)-tyrosine kinase inhibitors (TKIs) and other antitumor agents may delay drug resistance. In this study, we retrospectively reviewed the efficacy and safety of first-line concurrent EGFR-TKIs and platinum-based doublet chemotherapy with or without an antiangiogenic agent for advanced lung adenocarcinoma patients in the real world.
A total of 30 patients with advanced lung adenocarcinoma and activating EGFR mutations concurrently received an EGFR-TKI and platinum-based doublet chemotherapy with or without bevacizumab. The safety profile and efficacy were retrospectively reviewed.
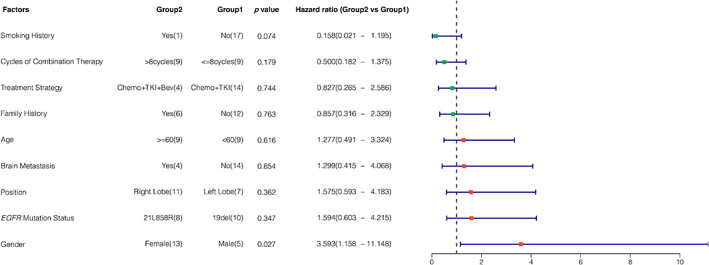
At the median follow-up time of 22.1 months, 18 patients had experienced disease progression, and six patients had died because of disease. The median progression-free survival (mPFS) was 21.2 months (95% CI: 12.631-29.798). Of the 28 patients who had measurable lesions, the objective response rate and disease control rate were 71.4% and 96.4%, respectively (one patient achieved complete remission, 19 patients had a partial response and seven patients had stable disease). Male patients had significantly longer mPFS than female patients (32.6 vs. 14.6 months, HR = 3.593, 95% CI: 1.158-11.148, p = 0.027). The most frequently seen grade 3/4 adverse events were hematological toxicities, seen in three cases (10%). Three patients ceased bevacizumab due to vascular events, including hypertension (grade 2, 6.7%) and venous thrombosis (grade 2, 3.3%), and continued EGFR-TKI and platinum-based doublet chemotherapy.
The combination of first-generation EGFR-TKIs with platinum-based chemotherapy may be a first-line treatment for advanced lung adenocarcinoma patients harboring activated EGFR mutations and is well tolerated.
先前的研究已经证实,表皮生长因子受体(EGFR)-酪氨酸激酶抑制剂(TKIs)与其他抗肿瘤药物联合使用可能会延缓耐药性的发生。在本研究中,我们回顾性分析了在真实世界中,一线同时使用 EGFR-TKI 和铂类双药化疗联合或不联合抗血管生成药物治疗晚期肺腺癌患者的疗效和安全性。
共 30 例晚期肺腺癌且携带激活型 EGFR 突变的患者同时接受 EGFR-TKI 和铂类双药化疗联合或不联合贝伐珠单抗治疗。回顾性分析安全性和疗效。
在中位随访时间 22.1 个月时,18 例患者发生疾病进展,6 例患者因疾病死亡。中位无进展生存期(mPFS)为 21.2 个月(95%CI:12.631-29.798)。在 28 例可测量病灶的患者中,客观缓解率和疾病控制率分别为 71.4%和 96.4%(1 例患者达到完全缓解,19 例患者部分缓解,7 例患者疾病稳定)。男性患者的 mPFS 明显长于女性患者(32.6 与 14.6 个月,HR=3.593,95%CI:1.158-11.148,p=0.027)。最常见的 3/4 级不良事件为血液学毒性,有 3 例(10%)。3 例患者因血管事件停止使用贝伐珠单抗,包括高血压(2 级,6.7%)和静脉血栓形成(2 级,3.3%),继续使用 EGFR-TKI 和铂类双药化疗。
第一代 EGFR-TKI 联合铂类化疗可能是晚期肺腺癌患者携带激活型 EGFR 突变的一线治疗方法,且具有良好的耐受性。