Department of Cardiology, Amsterdam Cardiovascular Sciences, Amsterdam UMC, Vrije Universiteit Amsterdam, De Boelelaan 1117, Amsterdam, 1081 HV, The Netherlands.
Department of Cardiology, Erasmus University Medical Center, Rotterdam, The Netherlands.
ESC Heart Fail. 2021 Oct;8(5):3726-3736. doi: 10.1002/ehf2.13444. Epub 2021 Jun 29.
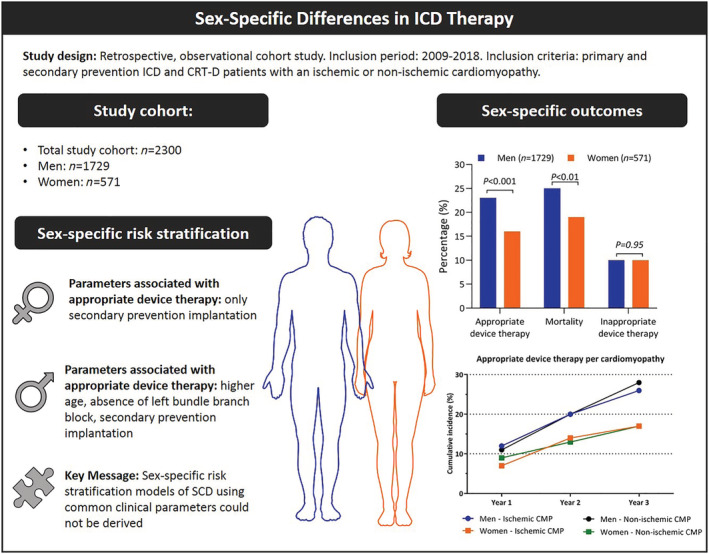
Risk stratification models of sudden cardiac death (SCD) are based on the assumption that risk factors of SCD affect risk to a similar extent in both sexes. The aim of the study is to evaluate differences in clinical outcomes between sexes and evaluate whether risk factors associated with appropriate device therapy (ADT) differ between men and women.
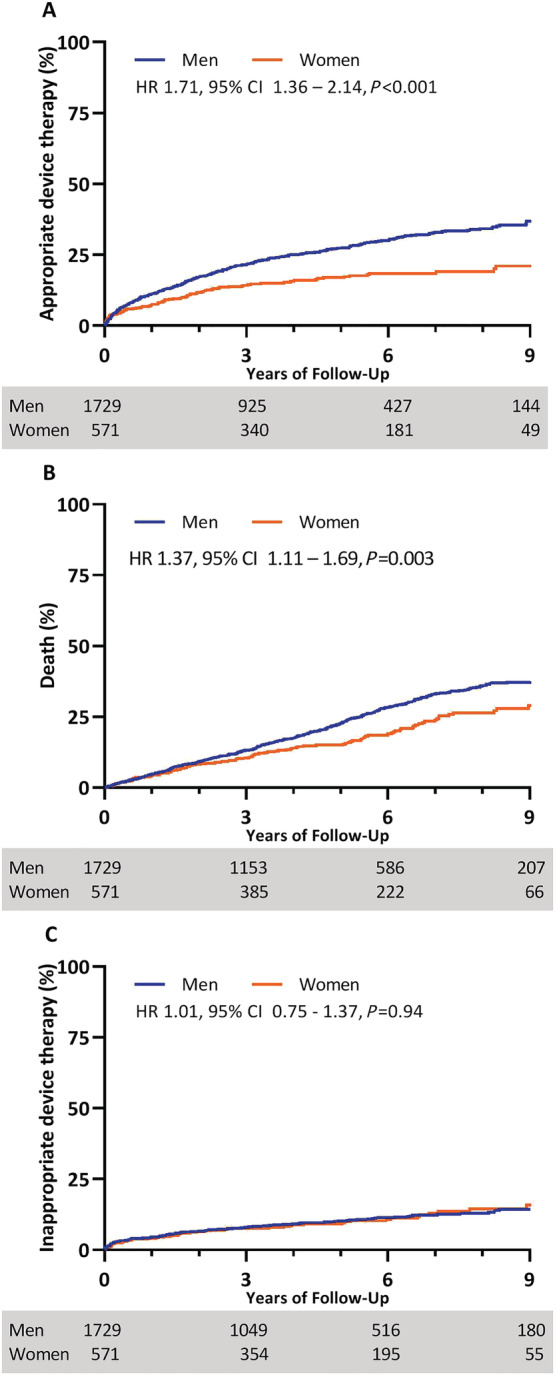
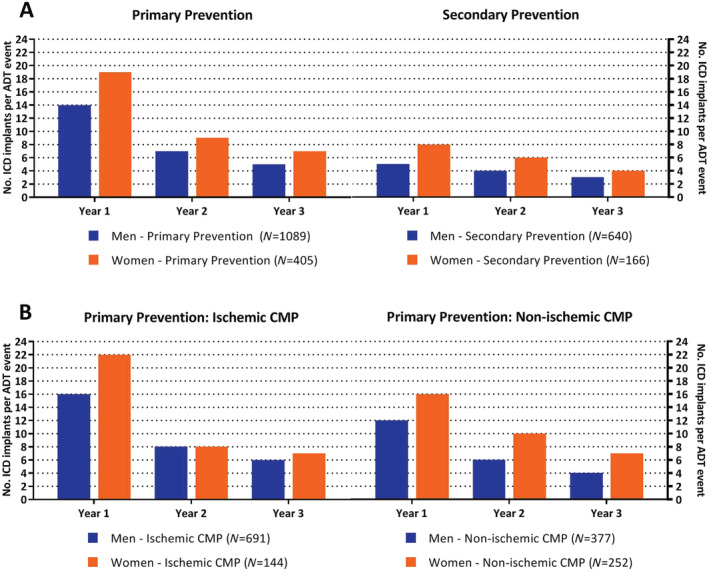
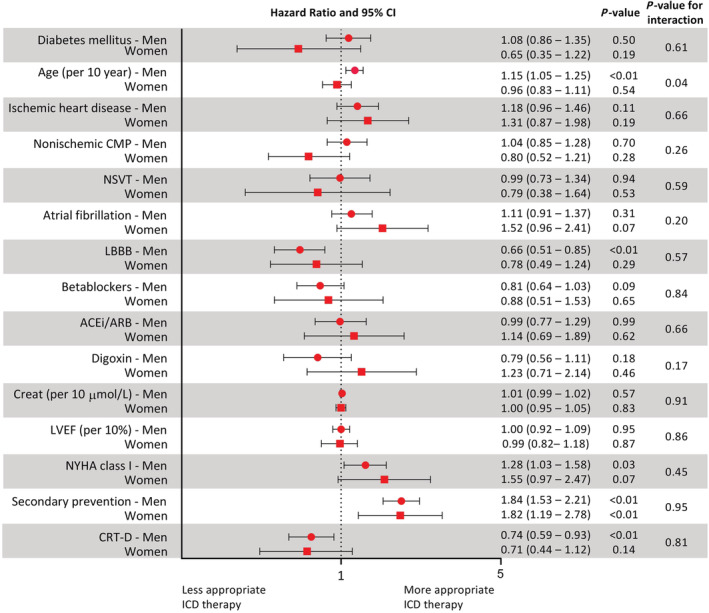
We performed a cohort study of implantable cardioverter defibrillator (ICD) patients referred for primary or secondary prevention of SCD between 2009 and 2018. Multivariable Cox regression models for prediction of ADT were constructed for men and women separately. Of 2300 included patients, 571 (25%) were women. Median follow-up was 4.6 (inter-quartile range: 4.4-4.9) years. Time to ADT was shorter for men compared with women [hazard ratio (HR) 1.71, P < 0.001], as was time to mortality (HR 1.37, P = 0.003). In women, only secondary prevention ICD therapy (HR 1.82, P < 0.01) was associated with ADT, whereas higher age (HR 1.20, P < 0.001), absence of left bundle branch block (HR 0.72, P = 0.01), and secondary prevention therapy (HR 1.80, P < 0.001) were independently associated with ADT in men. None of the observed parameters showed a distinctive sex-specific pattern in ADT.
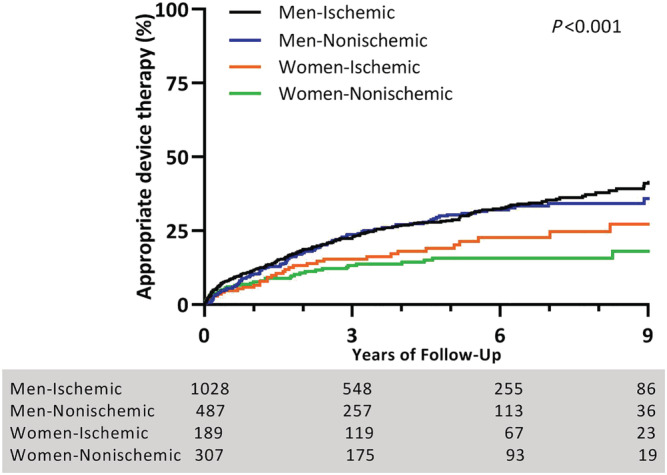
Male ICD patients were at higher risk of ADT and death compared with female ICD patients, irrespective of an ischaemic or non-ischaemic underlying cardiomyopathy. Our study highlights the importance to stratify outcomes of ICD trials by sex, as study results differ between men and women. However, none of the available clinical parameters showed a clear sex-specific relation to ventricular arrhythmias. As a consequence, sex-specific risk stratification models of SCD using commonly available clinical parameters could not be derived.
心脏性猝死(SCD)的风险分层模型基于这样一种假设,即 SCD 的危险因素对男性和女性的风险影响程度相似。本研究旨在评估两性之间临床结局的差异,并评估与适当器械治疗(ADT)相关的危险因素在男性和女性之间是否存在差异。
我们对 2009 年至 2018 年间因 SCD 进行一级或二级预防而植入植入式心律转复除颤器(ICD)的患者进行了一项队列研究。分别为男性和女性构建了 ADT 预测的多变量 Cox 回归模型。在纳入的 2300 例患者中,有 571 例(25%)为女性。中位随访时间为 4.6 年(四分位距:4.4-4.9)。与女性相比,男性 ADT 的时间更短[风险比(HR)1.71,P<0.001],死亡率的时间也更短(HR 1.37,P=0.003)。在女性中,只有二级预防 ICD 治疗(HR 1.82,P<0.01)与 ADT 相关,而年龄较高(HR 1.20,P<0.001)、无左束支传导阻滞(HR 0.72,P=0.01)和二级预防治疗(HR 1.80,P<0.001)与男性的 ADT 独立相关。在 ADT 中,观察到的参数均未表现出明显的性别特异性模式。
与女性 ICD 患者相比,男性 ICD 患者发生 ADT 和死亡的风险更高,无论是否存在缺血性或非缺血性心肌病。我们的研究强调了按性别分层 ICD 试验结果的重要性,因为男性和女性的研究结果存在差异。然而,现有的临床参数中没有一个与室性心律失常有明确的性别特异性关系。因此,无法使用常用的临床参数得出基于性别分层的 SCD 风险分层模型。