Sun Li, Li Juan, Li Xiaomeng, Yang Xuemei, Zhang Shujun, Wang Xue, Wang Nan, Xu Kanghong, Jiang Xinquan, Zhang Yi
School of Public Health, Shandong First Medical University & Shandong Academy of Medical Sciences, Taian, China.
Department of Clinical Laboratory, The Second Hospital, Cheeloo College of Medicine, Shandong University, Jinan, China.
Front Genet. 2021 Jun 14;12:676464. doi: 10.3389/fgene.2021.676464. eCollection 2021.
Recurrence remains the main cause of the poor prognosis in stage I-IIIA lung squamous cell carcinoma (LUSC) after surgical resection. In the present study, we aimed to identify the long non-coding RNAs (lncRNAs), microRNAs (miRNAs), and messenger RNAs (mRNAs) related to the recurrence of stage I-IIIA LUSC. Moreover, we constructed a risk assessment model to predict the recurrence of LUSC patients.
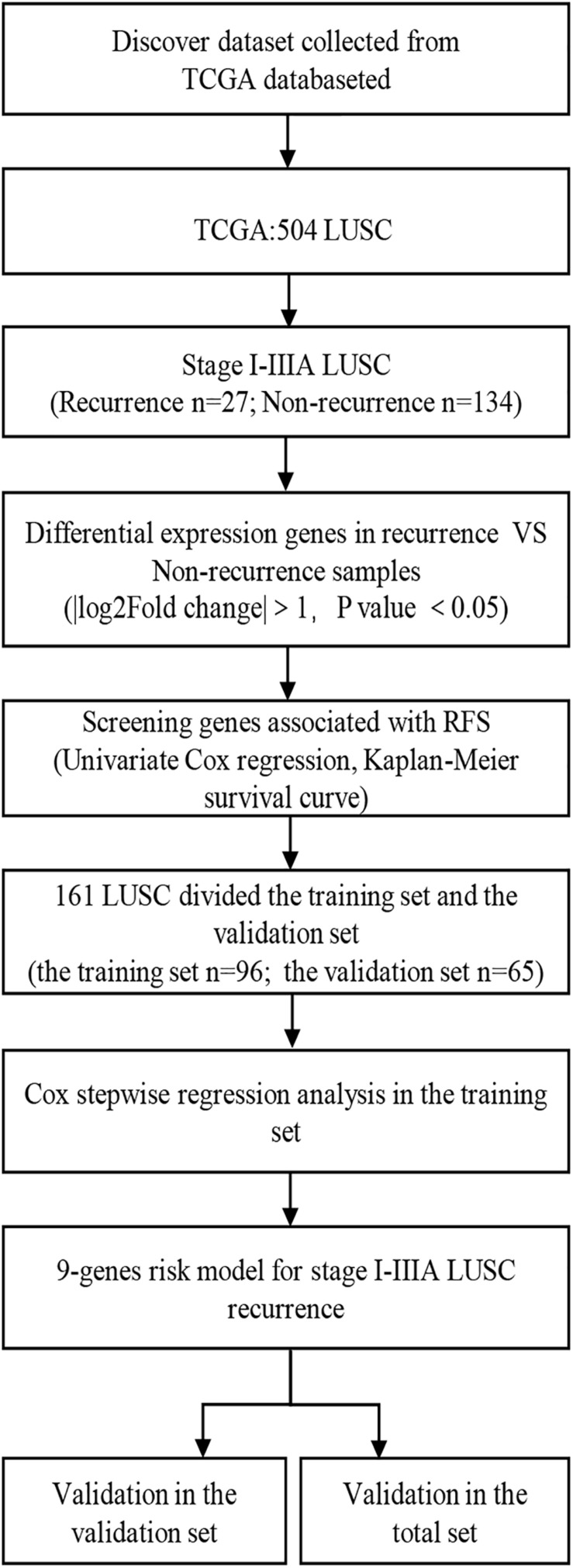
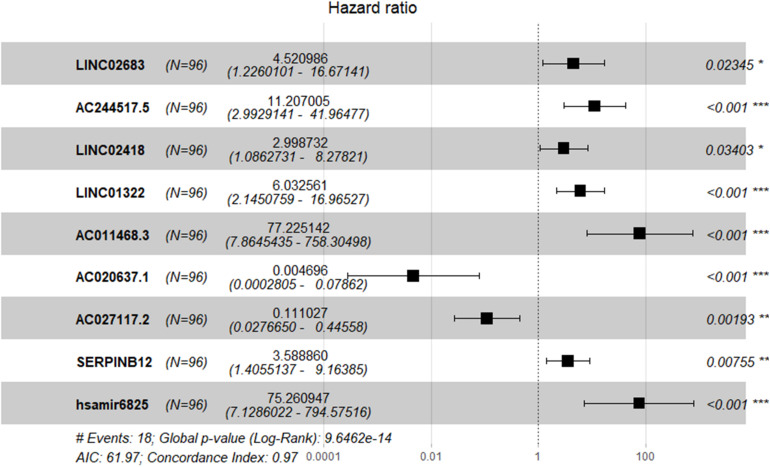
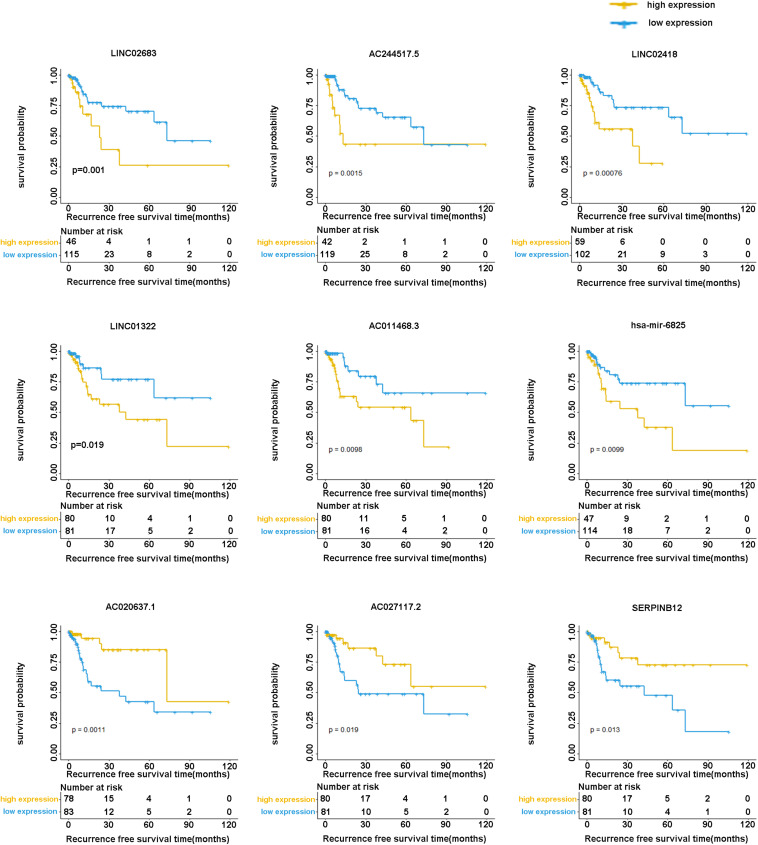
RNA sequencing data (including miRNAs, lncRNAs, and mRNAs) and relevant clinical information were obtained from The Cancer Genome Atlas (TCGA) database. The differentially expressed lncRNAs, miRNAs, and mRNAs were identified using the "DESeq2" package of the R language. Univariate Cox proportional hazards regression analysis and Kaplan-Meier curve were used to identify recurrence-related genes. Stepwise multivariate Cox regression analysis was carried out to establish a risk model for predicting recurrence in the training cohort. Moreover, Kaplan-Meier curves and receiver operating characteristic (ROC) curves were adopted to examine the predictive performance of the signature in the training cohort, validation cohort, and entire cohort.
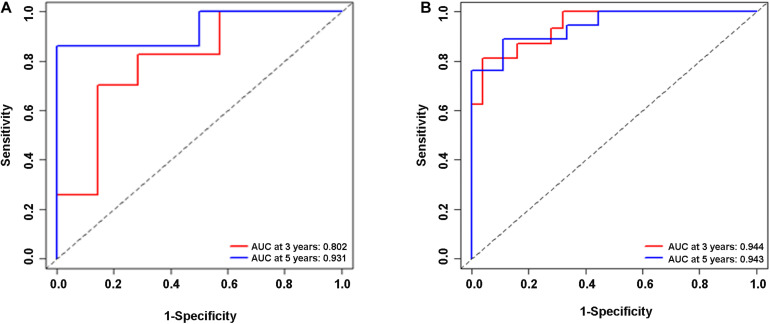
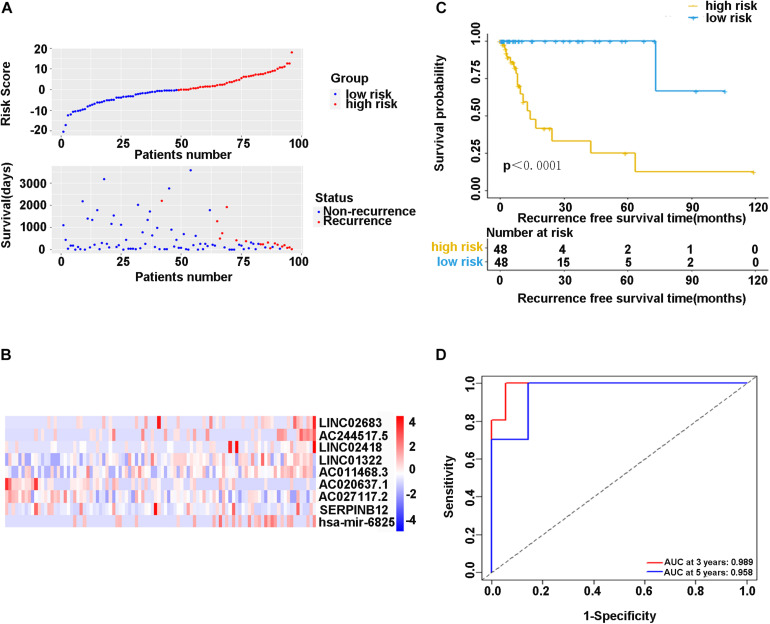
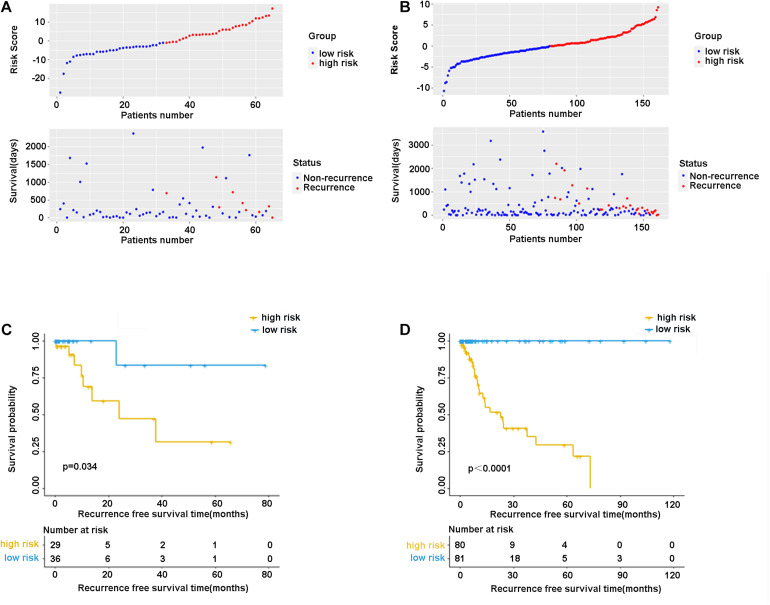
Based on the TCGA database, we analyzed the differentially expressed genes (DEGs) among 27 patients with recurrent stage I-IIIA LUSC and 134 patients with non-recurrent stage I-IIIA LUSC, and identified 431 lncRNAs, 36 miRNAs, and 746 mRNAs with different expression levels. Out of these DEGs, the optimal combination of DEGs was finally determined, and a nine-joint RNA molecular signature was constructed for clinical prediction of recurrence, including LINC02683, AC244517.5, LINC02418, LINC01322, AC011468.3, hsa-mir-6825, AC020637.1, AC027117.2, and SERPINB12. The ROC curve proved that the model had good predictive performance in predicting recurrence. The area under the curve (AUC) of the prognostic model for recurrence-free survival (RFS) was 0.989 at 3 years and 0.958 at 5 years (in the training set). The combined RNA signature also revealed good predictive performance in predicting the recurrence in the validation cohort and entire cohort.
In the present study, we constructed a nine-joint RNA molecular signature for recurrence prediction of stage I-IIIA LUSC. Collectively, our findings provided new and valuable clinical evidence for predicting the recurrence and targeted treatment of stage I-IIIA LUSC.
复发仍是I-IIIA期肺鳞状细胞癌(LUSC)手术切除后预后不良的主要原因。在本研究中,我们旨在鉴定与I-IIIA期LUSC复发相关的长链非编码RNA(lncRNA)、微小RNA(miRNA)和信使RNA(mRNA)。此外,我们构建了一个风险评估模型来预测LUSC患者的复发情况。
从癌症基因组图谱(TCGA)数据库中获取RNA测序数据(包括miRNA、lncRNA和mRNA)及相关临床信息。使用R语言的“DESeq2”软件包鉴定差异表达的lncRNA、miRNA和mRNA。采用单因素Cox比例风险回归分析和Kaplan-Meier曲线来鉴定复发相关基因。进行逐步多因素Cox回归分析以建立训练队列中预测复发的风险模型。此外,采用Kaplan-Meier曲线和受试者工作特征(ROC)曲线来检验该特征在训练队列、验证队列和整个队列中的预测性能。
基于TCGA数据库,我们分析了27例I-IIIA期LUSC复发患者和134例I-IIIA期LUSC未复发患者之间的差异表达基因(DEG),并鉴定出431个lncRNA、36个miRNA和746个mRNA具有不同的表达水平。在这些DEG中,最终确定了DEG的最佳组合,并构建了一个九联体RNA分子特征用于复发的临床预测,包括LINC02683、AC244517.5、LINC02418、LINC01322、AC011468.3、hsa-mir-6825、AC020637.1、AC027117.2和SERPINB12。ROC曲线证明该模型在预测复发方面具有良好的预测性能。复发-free生存(RFS)预后模型在3年时的曲线下面积(AUC)为0.989,5年时为0.958(在训练集中)。联合RNA特征在验证队列和整个队列中预测复发时也显示出良好的预测性能。
在本研究中,我们构建了一个用于I-IIIA期LUSC复发预测的九联体RNA分子特征。总体而言,我们的研究结果为预测I-IIIA期LUSC的复发和靶向治疗提供了新的有价值的临床证据。