Department of Neuromedicine and Movement Science, NTNU Norwegian University of Science and Technology, Edvard Griegs gate, Trondheim, Norway.
Division of Brain Sciences, Imperial College London, London, UK.
J Headache Pain. 2021 Jul 1;22(1):63. doi: 10.1186/s10194-021-01269-9.
The first manuscript in this series delineated a model of structured headache services, potentially cost-effective but requiring formal cost-effectiveness analysis (CEA). We envisaged a need for a new outcome measure for this purpose, applicable to all forms of treatment, care and care-delivery systems as opposed to comparisons of single-modality treatments.
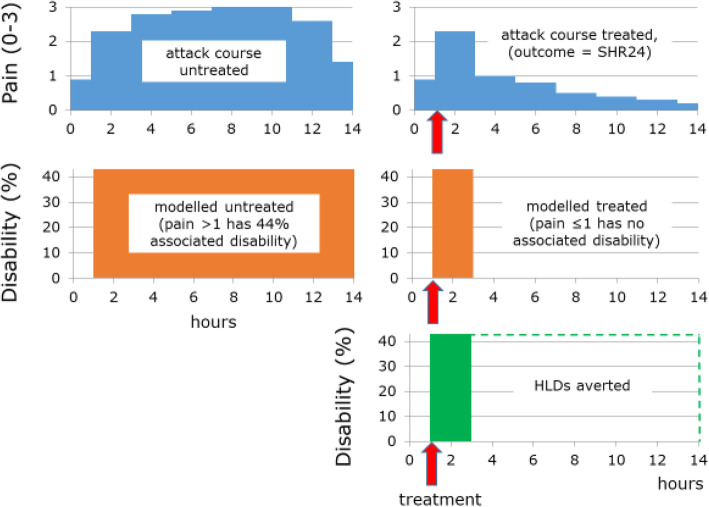
A literature review confirmed the lack of any suitable established measure. We prioritised construct validity, simplicity, comprehensiveness and expression in intuitive units. We noted that pain was the key burdensome symptom of migraine and episodic tension-type headache (TTH), that pain above a certain level was disabling, that it was difficult to put economic value to pain but relatively easy to do this for time, a casualty of headache leading to lost productivity. Alleviation of pain to a non-disabling level would be expected to bring restoration of function. We therefore based the measure on time spent in the ictal state (TIS) of migraine or TTH, either as total TIS or proportion of all time. We expressed impact on health, in units of time, as TISDW, where DW was the disability weight for the ictal state supplied by the Global Burden of Disease (GBD) studies. If the time unit was hours, TISDW yielded hours lived with (or lost to) disability (HLDs), in analogy with GBD's years lived with disability (YLDs).
Acute treatments would reduce TIS by shortening attack duration, preventative treatments by reducing attack frequency; health-care systems such as structured headache services would have these effects by delivering these treatments. These benefits were all measurable as HLDs-averted. Population-level estimates would be derived by factoring in prevalence, but also taking treatment coverage and adherence into account. For health-care systems, additional gains from provider-training (promoting adherence to guidelines and, therefore, enhancing coverage) and consumer-education (improving adherence to care plans), increasing numbers within populations gaining the benefits of treatments, would be measurable by the same metric.
The new outcome measure expressed in intuitive units of time is applicable to treatments of all modalities and to system-level interventions for multiple headache types, with utility for CEA and for informing health policy.
本系列的第一篇手稿阐述了一种结构化头痛服务模式,这种模式具有潜在的成本效益,但需要进行正式的成本效益分析(CEA)。我们设想为此需要一种新的结果衡量标准,适用于所有形式的治疗、护理和护理提供系统,而不是单一模式治疗的比较。
文献回顾证实,目前还没有任何合适的既定衡量标准。我们优先考虑结构有效性、简单性、全面性和直观单位的表达。我们注意到,疼痛是偏头痛和阵发性紧张型头痛(TTH)的主要负担症状,疼痛超过一定水平会导致残疾,对疼痛进行经济价值评估相对困难,但对时间进行评估相对容易,头痛导致生产力丧失的受害者。缓解疼痛至非致残水平预计将恢复功能。因此,我们将衡量标准建立在偏头痛或 TTH 的发作状态(TIS)上,既可以是总 TIS,也可以是所有时间的比例。我们用 TISDW 来衡量健康状况的影响,其中 DW 是全球疾病负担(GBD)研究提供的发作状态残疾权重。如果时间单位是小时,TISDW 会产生因残疾而丧失(或损失)的生活时间(HLDs),与 GBD 的残疾生活年(YLDs)类似。
急性治疗通过缩短发作持续时间来减少 TIS,预防治疗通过减少发作频率来减少 TIS;结构化头痛服务等医疗保健系统通过提供这些治疗来产生这些效果。这些收益都可以通过 HLDs 避免来衡量。通过考虑流行率,可以得出人群水平的估计,但还需要考虑治疗覆盖率和依从性。对于医疗保健系统,通过提供者培训(促进遵守指南,从而提高覆盖率)和消费者教育(改善对护理计划的依从性)所带来的额外收益,以及人群中获得治疗益处的人数增加,也可以通过同一指标来衡量。
以直观的时间单位表示的新结果衡量标准适用于所有模式的治疗和多种头痛类型的系统干预,对于 CEA 和为卫生政策提供信息具有实用性。