Mao Jimmy J, Baker Jessica E, Rainey William E, Young William F, Bancos Irina
Department of Medicine, Mayo Clinic, Rochester, MN, USA.
Department of Molecular & Integrative Physiology, University of Michigan, Ann Arbor, MI, USA.
J Endocr Soc. 2021 Jun 16;5(8):bvab107. doi: 10.1210/jendso/bvab107. eCollection 2021 Aug 1.
The detection and management of concomitant pheochromocytoma (PHEO) and primary aldosteronism (PA) is not well understood.
To investigate varying presentations and outcomes of cases with coexisting PHEO and PA to provide an approach to its diagnosis and management.
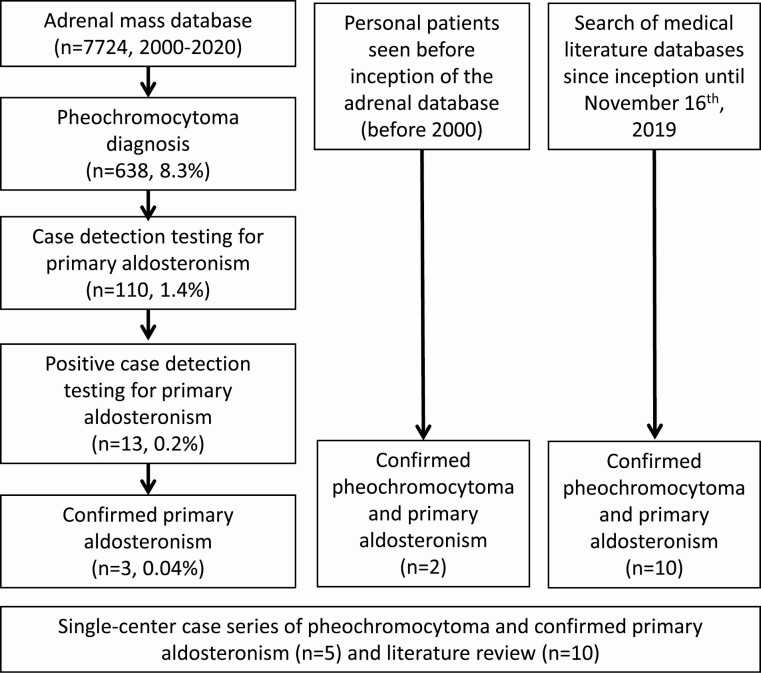
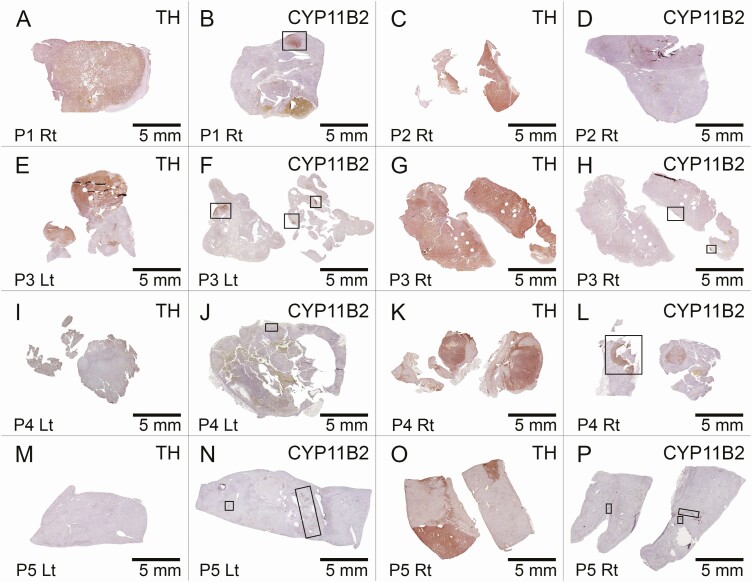
We conducted a retrospective case series of adult patients with concomitant PHEO and PA at Mayo Clinic from 2000-2020 and an additional review of cases before 2000 and from the medical literature. Clinical, biochemical, radiologic, and histologic parameters were measured.
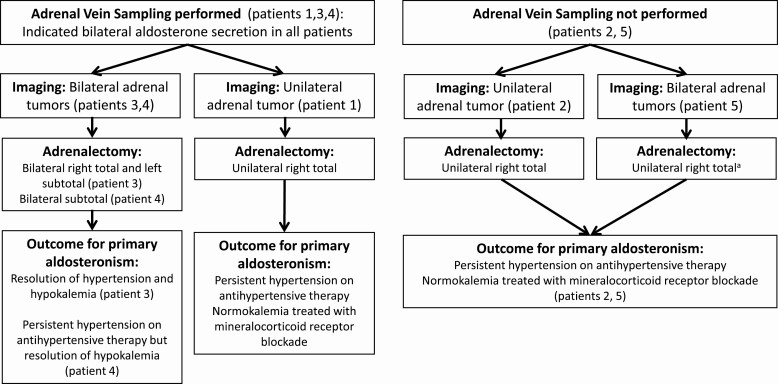
Fifteen patients (53% men, median age 53 years) were diagnosed with concomitant PHEO and PA. The majority presented with hypertension (13, 87%) and hypokalemia (13, 87%), and 6 (40%) presented with symptoms suggestive of catecholamine excess. All patients who underwent preoperative workup for catecholamine excess (14, 93%) were found to have biochemical levels above the upper limits of normal. Adrenal vein sampling (AVS) was performed in 9 patients (60%), where 5 (56%) were diagnosed with bilateral PA, and 4 (44%) with unilateral PA. Patients underwent either unilateral (12, 80%) or bilateral (3, 20%) adrenalectomy. Biochemical improvement or resolution of catecholamine excess was confirmed in all cases with documented measurements. Recurrence of PHEO was not observed. Six patients (40%) displayed persistent PA postoperatively.
Concomitant PHEO and PA is a rare but likely underreported condition. Hypertension with or without hypokalemia should prompt evaluation for PA, while any indeterminate adrenal mass should be assessed for PHEO. Coexisting disease warrants consideration of AVS to determine the laterality of PA to ensure appropriate management.
对于伴发嗜铬细胞瘤(PHEO)和原发性醛固酮增多症(PA)的检测与管理,目前了解尚少。
研究同时存在PHEO和PA的病例的不同表现及结局,以提供其诊断和管理方法。
我们对2000年至2020年在梅奥诊所就诊的成年伴发PHEO和PA患者进行了回顾性病例系列研究,并对2000年之前的病例及医学文献进行了额外回顾。测量了临床、生化、放射学和组织学参数。
15例患者(53%为男性,中位年龄53岁)被诊断为同时患有PHEO和PA。大多数患者表现为高血压(13例,87%)和低钾血症(13例,87%),6例(40%)表现出提示儿茶酚胺过量的症状。所有接受儿茶酚胺过量术前检查的患者(14例,93%)生化水平均高于正常上限。9例患者(60%)进行了肾上腺静脉采样(AVS),其中5例(56%)被诊断为双侧PA,4例(44%)为单侧PA。患者接受了单侧(12例,80%)或双侧(3例,20%)肾上腺切除术。所有有记录测量的病例均证实儿茶酚胺过量得到生化改善或缓解。未观察到PHEO复发。6例患者(40%)术后PA持续存在。
同时存在PHEO和PA是一种罕见但可能报告不足的情况。有或无低钾血症的高血压应促使对PA进行评估,而任何不确定的肾上腺肿块都应评估是否存在PHEO。并存疾病需要考虑进行AVS以确定PA的侧别,以确保适当的管理。