Endocrinology Service, Armed Forces Hospital, Lisboa, Portugal.
Imaging Service, Armed Forces Hospital, Lisboa, Portugal.
Am J Case Rep. 2023 Jun 27;24:e939659. doi: 10.12659/AJCR.939659.
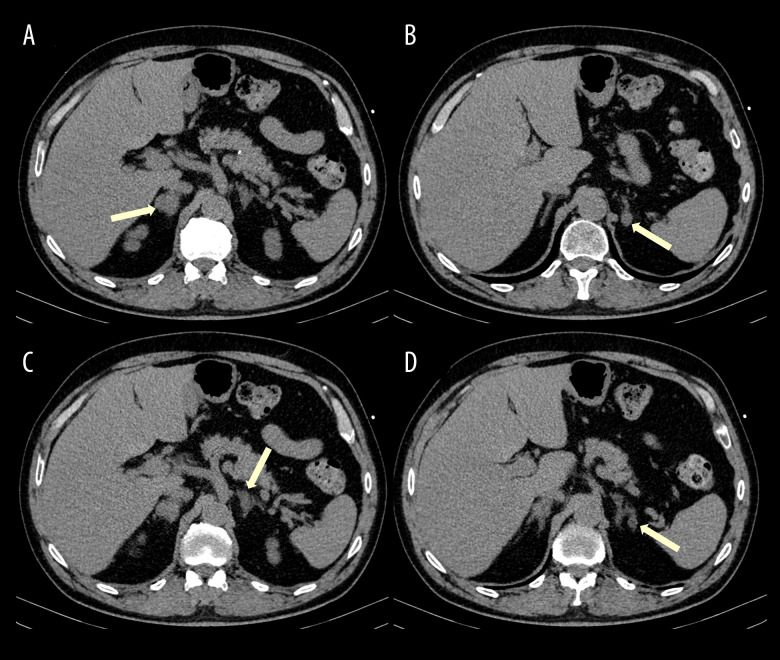
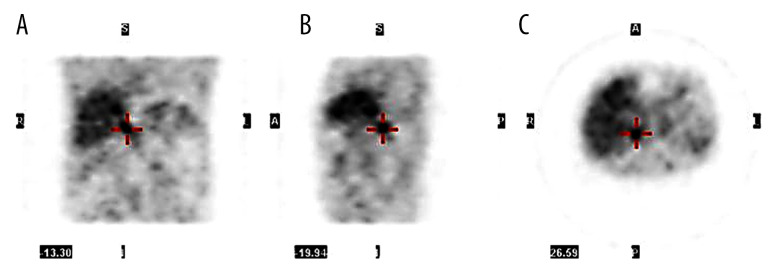
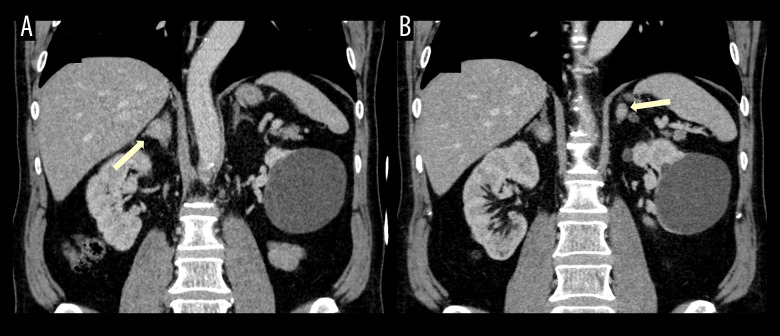
BACKGROUND Primary aldosteronism and pheochromocytoma are endocrine causes of secondary arterial hypertension. The association of primary aldosteronism and pheochromocytoma is rare and the involved mechanisms are poorly understood. Either there is a coexistence of both diseases or the pheochromocytoma stimulates the production of aldosterone. Since management approaches may differ significantly, it is important to properly diagnose the 2 conditions. We describe concomitant pheochromocytoma and primary aldosteronism in a patient with resistant hypertension, which demanded a challenging and individualized approach. CASE REPORT A 64-year-old man was sent for observation in our department for type 2 diabetes and resistant hypertension. Laboratory work-up suggested a primary aldosteronism and a pheochromocytoma. The abdominal CT (before and after intravenous contrast, with portal and delayed phase acquisitions) revealed an indeterminate right adrenal lesion and 3 nodules in the left adrenal gland: 1 indeterminate and 2 compatible with adenomas. A 18F-FDOPA PET-CT showed increased uptake in the right adrenal gland. The patient underwent a right adrenalectomy and a pheochromocytoma was confirmed. An improvement in glycemic control was observed after surgery but the patient remained hypertensive. A captopril test confirmed the persistence of primary aldosteronism, and he was started on eplerenone, achieving blood pressure control. CONCLUSIONS This case highlights the challenges in diagnosing and treating the simultaneous occurrence of pheochromocytoma and primary aldosteronism. Our main goal was surgical removal of the pheochromocytoma due to the risk of an adrenergic crisis.
原发性醛固酮增多症和嗜铬细胞瘤是继发性高血压的内分泌原因。原发性醛固酮增多症和嗜铬细胞瘤同时存在的情况很少见,其涉及的机制也知之甚少。可能同时存在这两种疾病,也可能是嗜铬细胞瘤刺激了醛固酮的产生。由于管理方法可能有很大差异,正确诊断这两种情况非常重要。我们描述了一位患有难治性高血压的患者同时存在嗜铬细胞瘤和原发性醛固酮增多症,这需要一种具有挑战性和个性化的方法。
一名 64 岁男性因 2 型糖尿病和难治性高血压被送到我们科室观察。实验室检查提示原发性醛固酮增多症和嗜铬细胞瘤。腹部 CT(静脉注射前后对比,包括门脉期和延迟期)显示右侧肾上腺有一个不确定的病变和左肾上腺的 3 个结节:1 个不确定,2 个符合腺瘤。18F-FDOPA PET-CT 显示右侧肾上腺摄取增加。患者接受了右侧肾上腺切除术,证实为嗜铬细胞瘤。手术后血糖控制得到改善,但患者仍有高血压。卡托普利试验证实原发性醛固酮增多症仍存在,开始使用依普利酮,血压得到控制。
本病例强调了诊断和治疗嗜铬细胞瘤和原发性醛固酮增多症同时存在的挑战。我们的主要目标是由于发生肾上腺素能危象的风险,手术切除嗜铬细胞瘤。