Roux Christian, Thomas Thierry, Paccou Julien, Bizouard Geoffray, Crochard Anne, Toth Emese, Lemaitre Magali, Maurel Frédérique, Perrin Laure, Tubach Florence
Department of Rheumatology Cochin Hospital, Assistance Publique - Hôpitaux de Paris Centre, Institut National de la Santé et de la Recherche Médicale (INSERM) Unités Mixtes de Recherche (UMR) 1153, Université de Paris Paris France.
Department of Rheumatology Hôpital Nord, Centre Hospitalier Universitaire (CHU) Saint-Etienne, INSERM U1059, Lyon University Saint-Etienne France.
JBMR Plus. 2021 May 14;5(7):e10507. doi: 10.1002/jbm4.10507. eCollection 2021 Jul.
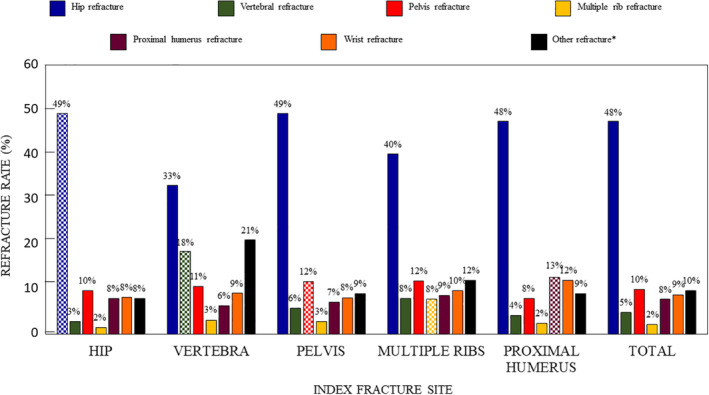
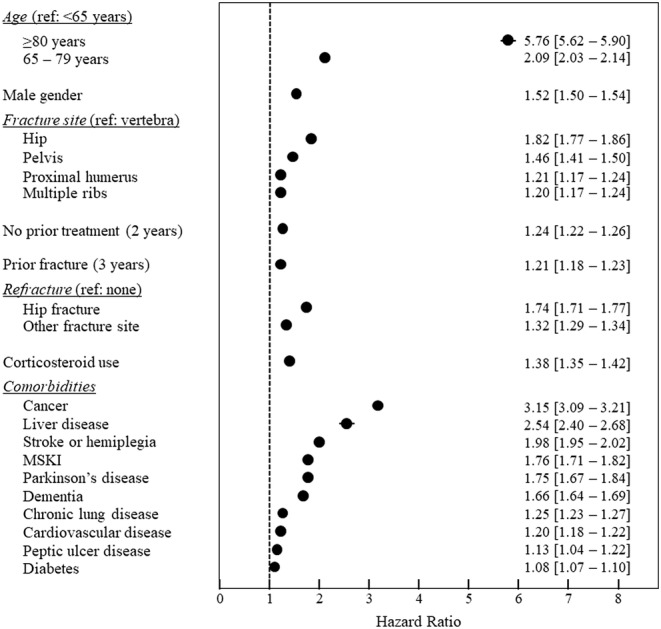
Severe osteoporotic fractures (hip, proximal humerus, pelvic, vertebral and multiple rib fractures) carry an increased risk of mortality. This retrospective cohort study in the French national healthcare database aimed to estimate refracture and mortality rates after severe osteoporotic fractures at different sites, and to identify mortality-related variables. A total of 356,895 patients hospitalized for severe osteoporotic fracture between 2009 and 2014 inclusive were analyzed. The cohort was followed for 2 to 8 years up to the study end or until the patient died. Data were extracted on subsequent hospitalizations, refracture events, treatments, comorbidities of interest and survival. Time to refracture and survival were described using Kaplan-Meier analysis by site of fracture and overall. Mortality risk factors were identified using a Cox model. Hip fractures accounted for 60.4% of the sample ( = 215,672). In the 12 months following fracture, 58,220 patients (16.7%) received a specific osteoporosis treatment, of whom 21,228 were previously treatment-naïve. The 12-month refracture rate was 6.3% (95% confidence interval [CI], 6.2%-6.3%), ranging from 4.0% (95% CI, 3.7%-4.3%) for multiple rib fractures to 7.8% (95% CI, 7.5%-8.1%) for pelvic fractures. Twelve-month all-cause mortality was 12.8% (95% CI, 12.7%-12.9%), ranging from 5.0% (95% CI, 4.7%-5.2%) for vertebral fractures to 16.6% (95% CI, 16.4%-16.7%) for hip fractures. Osteoporosis-related mortality risk factors included fracture site, previous osteoporotic fracture (hazard ratio 1.21; 95% CI, 1.18-1.23), hip refracture (1.74; 95% CI, 1.71-1.77), and no prior osteoporosis treatment (1.24; 95% CI, 1.22-1.26). Comorbid cancer (3.15; 95% CI, 3.09-3.21) and liver disease (2.54; 95% CI, 2.40-2.68) were also strongly associated with mortality. In conclusion, severe osteoporotic fractures, including certain non-hip nonvertebral fractures, carry a high burden in terms of mortality and refracture risk. However, most patients received no anti-osteoporotic treatment. The findings emphasize the importance of better management of patients with severe fractures, and of developing effective strategies to reduce fracture risk in patients with osteoporosis. © 2021 The Authors. published by Wiley Periodicals LLC on behalf of American Society for Bone and Mineral Research.
严重骨质疏松性骨折(髋部、肱骨近端、骨盆、椎体和多发性肋骨骨折)会增加死亡风险。这项在法国国家医疗数据库中开展的回顾性队列研究旨在估算不同部位严重骨质疏松性骨折后的再骨折率和死亡率,并确定与死亡相关的变量。对2009年至2014年(含)期间因严重骨质疏松性骨折住院的356,895例患者进行了分析。对该队列随访2至8年,直至研究结束或患者死亡。提取了关于后续住院情况、再骨折事件、治疗、感兴趣的合并症和生存情况的数据。采用Kaplan-Meier分析按骨折部位和总体情况描述再骨折时间和生存情况。使用Cox模型确定死亡风险因素。髋部骨折占样本的60.4%(n = 215,672)。在骨折后的12个月内,58,220例患者(16.7%)接受了特定的骨质疏松治疗,其中21,228例此前未接受过治疗。12个月时的再骨折率为6.3%(95%置信区间[CI],6.2%-6.3%),范围从多发性肋骨骨折的4.0%(95%CI,3.7%-4.3%)到骨盆骨折的7.8%(95%CI,7.5%-8.1%)。12个月时的全因死亡率为12.8%(95%CI,12.7%-12.9%),范围从椎体骨折的5.0%(95%CI,4.7%-5.2%)到髋部骨折的16.6%(95%CI,16.4%-16.7%)。与骨质疏松相关的死亡风险因素包括骨折部位、既往骨质疏松性骨折(风险比1.21;95%CI,1.18-1.23)、髋部再骨折(1.74;95%CI,1.71-1.77)以及既往未接受过骨质疏松治疗(1.24;95%CI,1.22-1.26)。合并癌症(3.15;95%CI,3.09-3.21)和肝病(2.54;95%CI,2.40-2.68)也与死亡密切相关。总之,严重骨质疏松性骨折,包括某些非髋部非椎体骨折,在死亡率和再骨折风险方面负担沉重。然而,大多数患者未接受抗骨质疏松治疗。这些发现强调了更好地管理严重骨折患者以及制定有效策略降低骨质疏松患者骨折风险 的重要性。© 2021作者。由Wiley Periodicals LLC代表美国骨与矿物质研究学会出版。