Kahana-Edwin Smadar, Cain Lucy E, McCowage Geoffrey, Darmanian Artur, Wright Dale, Mullins Anna, Saletta Federica, Karpelowsky Jonathan
Advanced Molecular Diagnostics, Children's Cancer Research Unit, Kids Research, The Children's Hospital at Westmead, Sydney, NSW 2145, Australia.
Cancer Centre for Children, The Children's Hospital at Westmead, Sydney, NSW 2145, Australia.
Cancers (Basel). 2021 Jul 5;13(13):3365. doi: 10.3390/cancers13133365.
amplification (MNA), segmental chromosomal aberrations (SCA) and activating mutations are biomarkers for risk-group stratification and for targeted therapeutics for neuroblastoma, both of which are currently assessed on tissue biopsy. Increase in demand for tumor genetic testing for neuroblastoma diagnosis is posing a challenge to current practice, as the small size of the core needle biopsies obtained are required for multiple molecular tests. We evaluated the utility of detecting these biomarkers in the circulation.
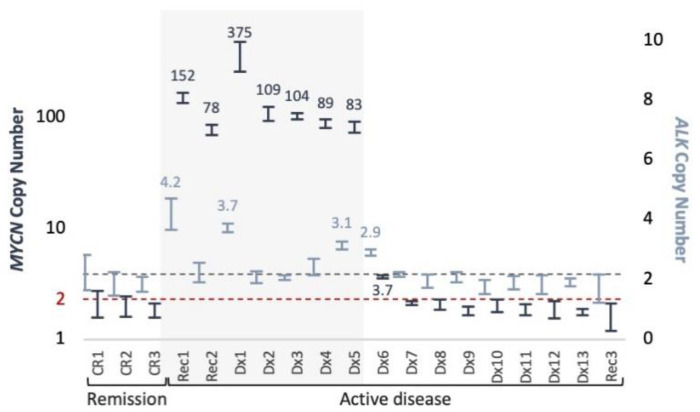
Various pre-analytical conditions tested to optimize circulating-tumor DNA (ctDNA) copy number changes evaluations. Plasma samples from 10 patients diagnosed with neuroblastoma assessed for SCA and MNA using single nucleotide polymorphism (SNP) array approach currently used for neuroblastoma diagnosis, with MNA status assessed independently using digital-droplet PCR (ddPCR). Three patients (one in common with the previous 10) tested for activating mutations p.F1174L and p.F1245I using ddPCR.
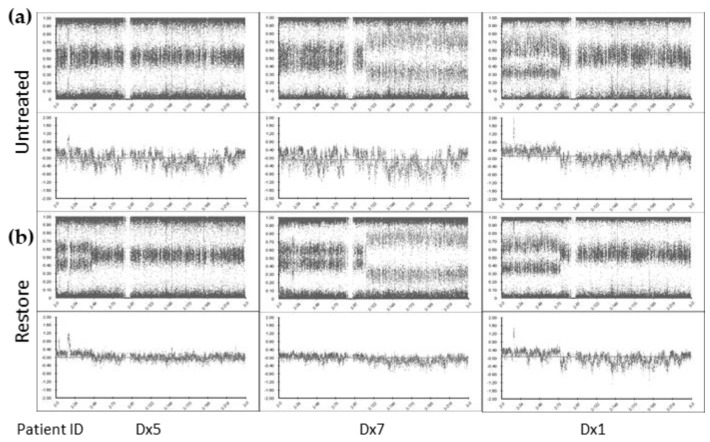
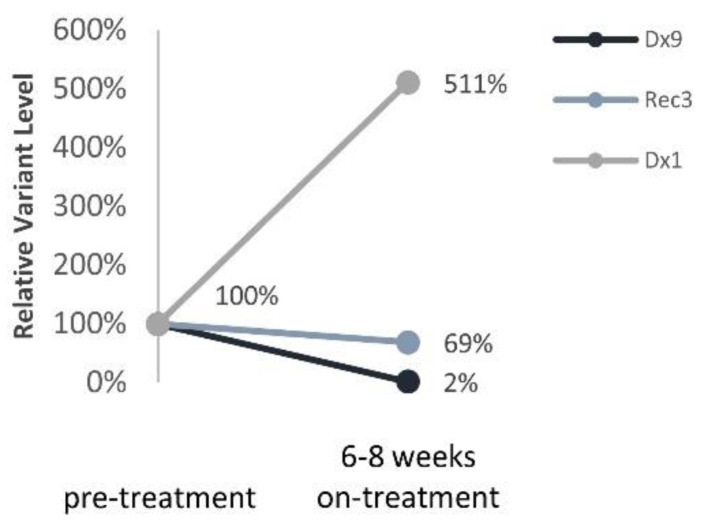
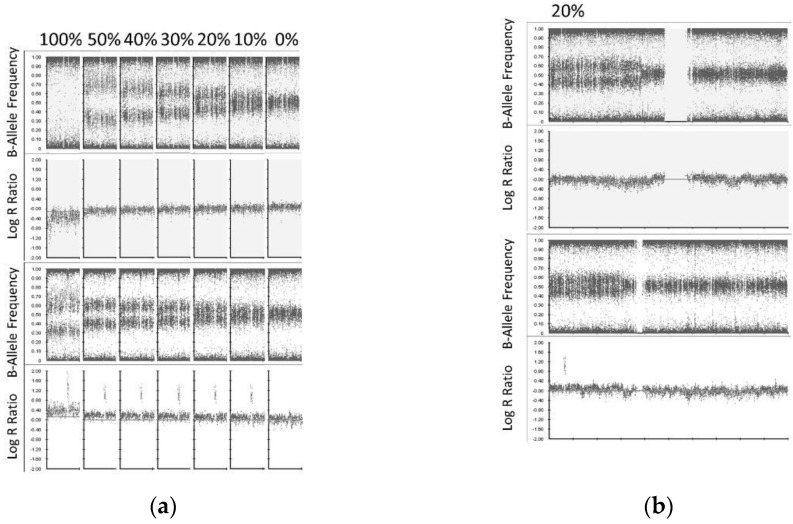
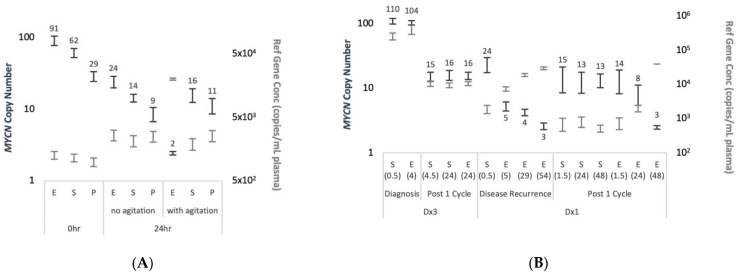
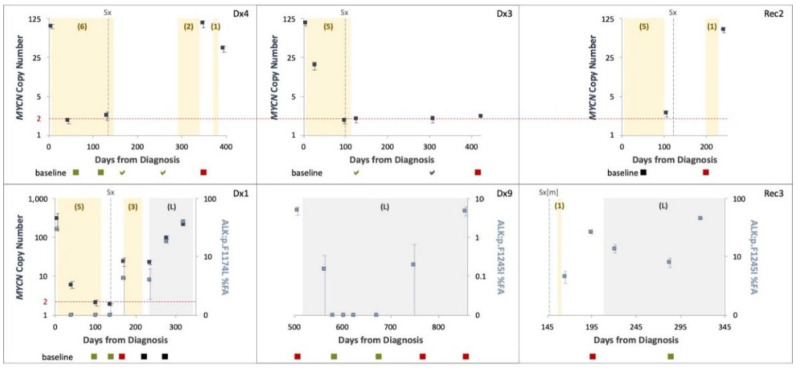
Copy number detection is highly affected by physical perturbations of the blood sample (mimicking suboptimal sample shipment), which could be overcome using specialized preservative collection tubes. Pre-analytical DNA repair procedures on ctDNA before SNP chromosome microarray processing improved the lower limit of detection for SCA and MNA, defined as 20% and 10%, respectively. We detected SCA in 10/10 (100%) patients using SNP array, 7 of which also presented MNA. Circulating-free DNA (cfDNA) and matched tumor DNA profiles were generally identical. MNA was detected using ddPCR in 7/7 (100%) of MNA and 0/12 (0%) non-MNA cases. MNA and mutation dynamic change was assessed in longitudinal samples from 4 and 3 patients (one patient with both), respectively, accurately reflected response to treatment in 6/6 (100%) and disease recurrence in 5/6 (83%) of cases. Samples taken prior to targeted treatment with the ALK inhibitor Lorlatinib and 6-8 weeks on treatment showed reduction/increase in variants according to response to treatment.
These results demonstrate the feasibility of ctDNA profiling for molecular risk-stratification, and treatment monitoring in a clinically relevant time frame and the potential to reduce fresh tissue requirements currently embedded in the management of neuroblastoma.
基因扩增(MNA)、节段性染色体畸变(SCA)和激活突变是神经母细胞瘤风险分层和靶向治疗的生物标志物,目前这两者均通过组织活检进行评估。神经母细胞瘤诊断对肿瘤基因检测的需求增加,这给当前的实践带来了挑战,因为获取的芯针活检组织样本较小,而多项分子检测都需要使用这些样本。我们评估了在循环系统中检测这些生物标志物的效用。
测试了各种分析前条件,以优化循环肿瘤DNA(ctDNA)拷贝数变化评估。对10例诊断为神经母细胞瘤的患者的血浆样本,使用目前用于神经母细胞瘤诊断的单核苷酸多态性(SNP)阵列方法评估SCA和MNA,并使用数字液滴PCR(ddPCR)独立评估MNA状态。对3例患者(其中1例与之前的10例患者相同)使用ddPCR检测激活突变p.F1174L和p.F1245I。
拷贝数检测受血样物理扰动(模拟次优样本运输)的影响很大,使用专门的防腐剂收集管可以克服这一问题。在进行SNP染色体微阵列处理之前,对ctDNA进行分析前DNA修复程序可提高SCA和MNA的检测下限,分别定义为20%和10%。我们使用SNP阵列在10/10(100%)的患者中检测到SCA,其中7例还存在MNA。游离循环DNA(cfDNA)和匹配的肿瘤DNA谱通常相同。在7/7(100%)的MNA病例和0/12(0%)的非MNA病例中,使用ddPCR检测到MNA。分别对4例和3例患者(1例患者同时涉及两者)的纵向样本评估MNA和突变动态变化,在6/6(100%)的病例中准确反映了对治疗的反应,在5/6(83%)的病例中反映了疾病复发。在使用ALK抑制剂劳拉替尼进行靶向治疗前以及治疗6 - 8周时采集的样本显示,根据治疗反应,变异体减少/增加。
这些结果证明了ctDNA分析用于分子风险分层和在临床相关时间框架内进行治疗监测的可行性,以及减少目前神经母细胞瘤管理中对新鲜组织需求的潜力。