Li Xiaofei, Zhang Junmeng, Qiu Chunguang, Wang Zhao, Li Hui, Pang Kunjing, Yao Yan, Liu Zhimin, Xie Ruiqin, Chen Yangxin, Wu Yongquan, Fan Xiaohan
Department of Cardiology, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China.
Department of Cardiology, Beijing Anzhen Hospital, Capital Medical University, Beijing, China.
Front Cardiovasc Med. 2021 Jul 8;8:685253. doi: 10.3389/fcvm.2021.685253. eCollection 2021.
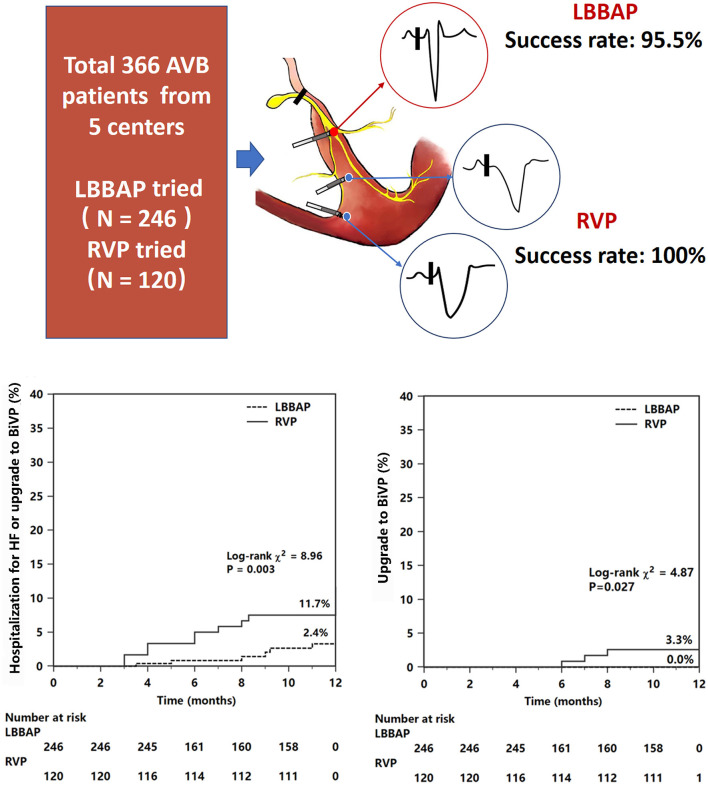
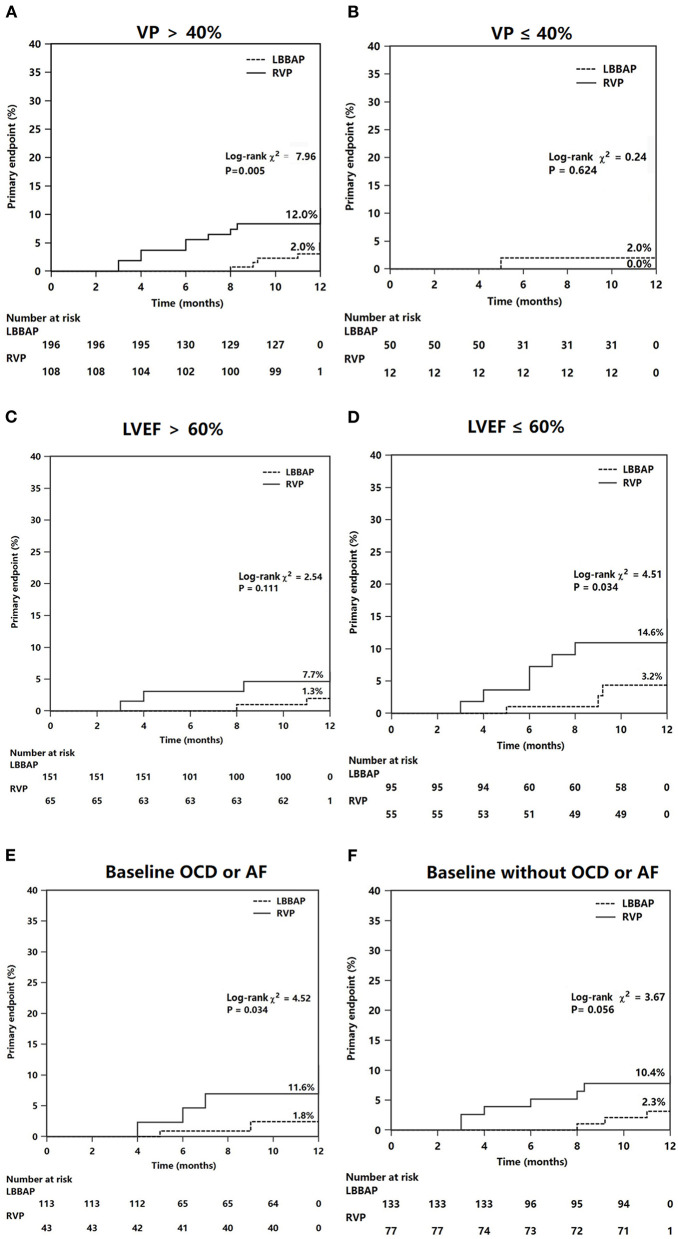
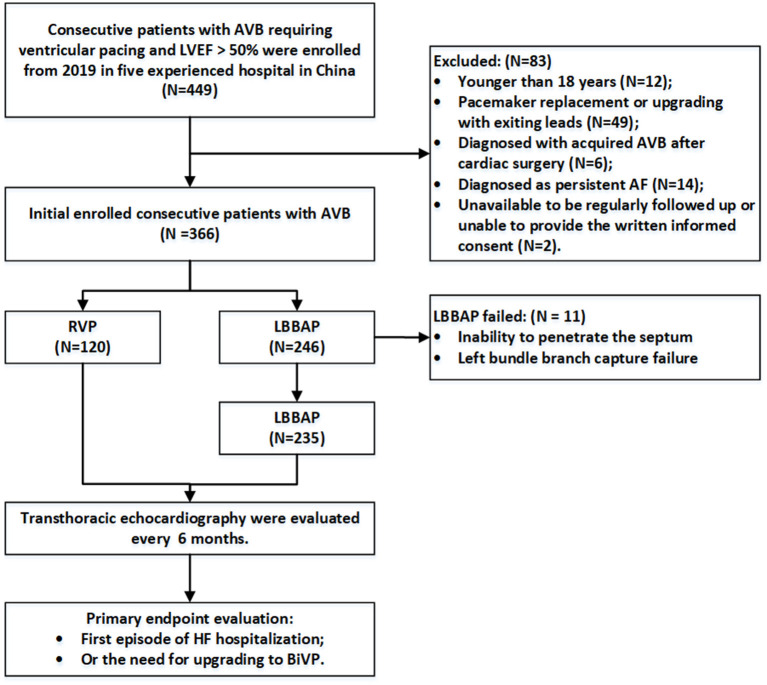
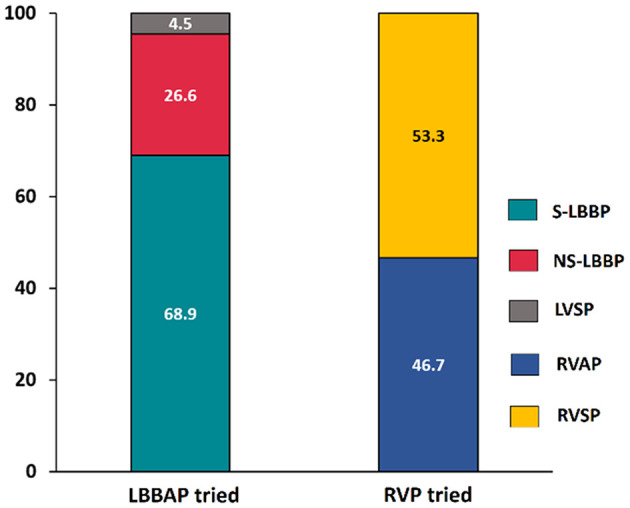
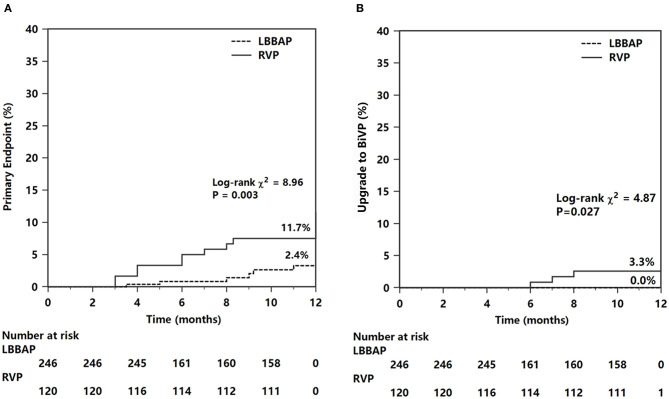
Left bundle branch area pacing (LBBAP) is a novel pacing modality with stable pacing parameters and a narrow-paced QRS duration. We compared heart failure (HF) hospitalization events and echocardiographic measures between LBBAP and right ventricular pacing (RVP) in patients with atrioventricular block (AVB). This multicenter observational study prospectively recruited consecutive AVB patients requiring ventricular pacing in five centers if they received LBBAP or RVP and had left ventricular ejection fraction (LVEF) >50%. Data on electrocardiogram, pacing parameters, echocardiographic measurements, device complications, and clinical outcomes were collected at baseline and during follow-up. The primary outcome was first episode hospitalization for HF or upgrade to biventricular pacing. LBBAP was successful in 235 of 246 patients (95.5%), while 120 patients received RVP. During a mean of 11.4 ± 2.7 months of follow-up, the ventricular pacing burden was comparable (83.9 ± 35.1 vs. 85.7 ± 30.0%), while the mean LVEF differed significantly (62.6 ± 4.6 vs. 57.8 ± 11.4%) between the LBBAP and RVP groups. Patients with LBBAP had significantly lower occurrences of HF hospitalization and upgrading to biventricular pacing than patients with RVP (2.6 vs. 10.8%, <0.001), and differences in primary outcome between LBBAP and RVP were mainly observed in patients with ventricular pacing >40% or with baseline LVEF <60%. The primary outcome was independently associated with LBBAP (adjusted HR 0.14, 95% CI: 0.04-0.55), previous myocardial infarction (adjusted HR 6.82, 95% CI: 1.23-37.5), and baseline LVEF (adjusted HR 0.91, 95% CI: 0.86-0.96). Permanent LBBAP might reduce the risk of HF hospitalization or upgrade to biventricular pacing compared with RVP in AVB patients requiring a high burden of ventricular pacing. URL: https://www.clinicaltrials.gov; Unique identifier: NCT03851315; URL: http://www.chictr.org.cn; Unique Identifier: ChiCTR2100043296.
左束支区域起搏(LBBAP)是一种新型起搏方式,起搏参数稳定,起搏QRS波时限窄。我们比较了房室传导阻滞(AVB)患者中LBBAP与右心室起搏(RVP)的心力衰竭(HF)住院事件及超声心动图测量结果。这项多中心观察性研究前瞻性纳入了五个中心连续的需要心室起搏的AVB患者,这些患者接受LBBAP或RVP且左心室射血分数(LVEF)>50%。在基线期和随访期间收集心电图、起搏参数、超声心动图测量、器械并发症及临床结局的数据。主要结局是首次因HF住院或升级为双心室起搏。246例患者中有235例(95.5%)LBBAP成功,120例患者接受RVP。在平均11.4±2.7个月的随访期间,LBBAP组与RVP组的心室起搏负担相当(83.9±35.1%对85.7±30.0%),但平均LVEF差异显著(62.6±4.6%对57.8±11.4%)。LBBAP组患者的HF住院及升级为双心室起搏的发生率显著低于RVP组患者(2.6%对10.8%,<0.001),LBBAP与RVP在主要结局上的差异主要在心室起搏>40%或基线LVEF<60%的患者中观察到。主要结局与LBBAP(校正HR 0.14,95%CI:0.04 - 0.55)、既往心肌梗死(校正HR 6.82,95%CI:1.23 - 37.5)及基线LVEF(校正HR 0.91,95%CI:0.86 - 0.96)独立相关。与RVP相比,对于需要高心室起搏负担的AVB患者,永久性LBBAP可能降低HF住院或升级为双心室起搏的风险。网址:https://www.clinicaltrials.gov;唯一标识符:NCT03851315;网址:http://www.chictr.org.cn;唯一标识符:ChiCTR2100043296。